Biomedica - Official Journal of University of Health Sciences, Lahore, Pakistan
Volume 38(4):225-229
ORIGINAL ARTICLE
Agreement between arterial and venous blood gas measurements in patients with sepsis and septic shock
Abida Pervaiz1*  , Sadia Bashir2, Zareen Gulrohi3, Usman Pasha4, Xiao Ning5, Khalid Mehmud Khan1
, Sadia Bashir2, Zareen Gulrohi3, Usman Pasha4, Xiao Ning5, Khalid Mehmud Khan1
Received: 21 August 2022 Revised date: 24 November 2022 Accepted: 13 December 2022
Correspondence to: Abida Pervaiz
*Senior Registrar, Department of Medicine, Jinnah Hospital Lahore, Lahore, Pakistan.
Email: abiam22@gmail.com
Full list of author information is available at the end of the article.
ABSTRACT
Background and Objective:
Acid–base status is mandatory for clinical assessment of patients with septic shock and severe sepsis. Generally, venous blood gas sample collection is easier, however, the data regarding this approach are lesser defined in our population as a substitute for arterial blood gas (ABG) sample. The present study aimed to determine and compare the pH, pCO2, and bicarbonate levels in VBG and ABG samples in patients with sepsis and septic shock.
Method:
A cross sectional comparative study was conducted on 350 patients with sepsis and/or septic shock admitted to the medical emergency of Jinnah Hospital, Lahore, Pakistan. Both ABG and VBG samples were collected and pH, pCO2, and bicarbonate levels were determined by standard methods. Data were analyzed using Pearson correlation and the Bland–Altman method for bias.
Results:
An interclass correlation (r = 0.995, r = 0.929 and r = 0.946) was found for pH, pCO2, and bicarbonate between ABG and VBG samples, respectively. The Bland–Altman method showed a high degree of agreement for two sets of measurements; pH (bias ± SD, 0.089 ± 0.00472) and pCO2 (bias ± SD, -1.1096 ± 1.0089) with a clinically acceptable difference whereas the difference in bicarbonate measurement was found slightly higher (bias ± SD, 1.124 ± 0.674) revealing, however, a good degree of agreement with clinically acceptable bias.
Conclusion:
Use of a venous blood sample in patients with sepsis or septic shock is a clinically acceptable substituent for ABG measurement in evaluating acid-base status of these patients for further management.
Keywords:
Sepsis, septic shock, arterial blood gases, venous blood gases, agreement, bias.
Introduction
Sepsis is a heterogeneous disorder characterized by acute organ dysfunction, acute kidney, and/or respiratory failure, severe metabolic disturbances and a high risk of death because of unbalanced host response against infection; thus, urgent treatment and management are mandatory.1,2 Despite advancement in therapeutic options, it is still a disorder with one of the highest occurrence and death rates worldwide thus making it a significant public health issue with substantial economic implications.3,4 Sepsis was identified as a global health priority by World Health Assembly and World Health Organization in 2017 and a resolution was approved to reinforce its timely diagnosis, treatment as well as prevention.5
Acid–base analysis is believed to be an important outcome in the critical care medicine that provides critical information on a variety of diseases. Traditionally, arterial blood gas (ABG) has been used as a gold standard method to determine the patient’s acid-base status; however, venous blood samples are commonly obtained for other biochemical or hematological measurements. The potential risks of collecting ABG sample included thrombosis or embolization, discomfort, hematoma formation, chances of aneurysm development, needle stick injuries to medical personnel, and occasionally even reflex sympathetic dystrophy.6 Contrary to this, collection of venous blood gas (VBG) sample is easier, lesser time taking and is useful for determining other clinical investigations on a single sample.7 Several researchers have investigated regarding the usefulness of VBG as a substituent for ABG sample and reported a significant correlation or agreement between ABG and VBG in various diseases including acute respiratory failure,6,8 diabetic ketoacidosis,9 trauma,10 chronic obstructive pulmonary disease,11,12 cardiac arrest,13 and other critical disorders with unknown origin.14 Keeping in view the significance of these investigations, there is a need to assess the acid-base status in patients with sepsis and/or septic shock comparing ABG and VBG samples. The present study aimed to find out a probable correlation or agreement between ABG and VBG measurements for the clinical management of patients with sepsis and/or septic shock in local population.
Methods
A cross sectional comparative study was conducted at the Department of Medicine (DOM), Jinnah hospital, Lahore, Pakistan, following the amended Declaration of Helsinki and was fully approved from institutional review board. A total of 350 patients presenting to the emergency department with ages ranging from 30-60 years and who clinically fulfilled the criteria of sepsis and/or septic shock were recruited for the study after taking written informed consent from the patient or related attendants in case of compromised consciousness. Patients with hypovolemic shock, cardiopulmonary arrest, pregnancy, and/or those not willing for dual puncture were excluded from the study.
Simultaneously, blood gas samples (ABG and VBG) were taken within the first 24-48 hours after admission. Both samples were sequentially taken in standard blood gas syringes within a time frame of no longer than 15 minutes. The ABG sample was collected using an artery catheter or a needle puncture while the VBG sample was collected from peripheral veins. All blood gas samples were taken by clinical staff using standard protocol for blood gas collection followed by transportation to central laboratory in ice for analysis.
Statistical analysis
Demographic and clinical information were recorded and clinical information (pH, pCO2, and bicarbonate) were measured and reported as descriptive statistics [mean, standard deviation (SD)], frequencies, and range using SPSS software for windows, version 21.0. (SPSS Inc., Chicago, IL). For interclass agreement [interclass correlation (ICC)], correlation analysis was executed for pH, pCO2, and bicarbonates in ABG and VBG samples while Bland-Altman agreement was used for agreement between the two blood gas types.
With an expected mean difference of 0.80, a sample size of 350 was required to achieve a 95% confidence interval for each limit of agreement (LOA) between pCO2 measured from venous and ABG. With a significance level of 0.05, it was predicted that this sample size would have 81% power to identify an ICC of 0.8 under the alternative hypothesis while the ICC under the null hypothesis is 0.7.
Results
During the study period, 1,578 patients were admitted to DOM and 350 patients who met the inclusion criteria were selected. Amongst the 350 enrolled patients, 156 (44.6%) were females and 194 (55.4%) were males with a mean age of 48.06 ± 8.895 years. Demographic and clinical information were recorded and are summarized in Table 1.
The commonest comorbidities observed were Hepatitis B & C in 77 (22%) followed by diabetes mellitus in 72 (20.6%) patients. The arterial sample pH ranged from 7.102 to 7.550 in comparison with that of venous sample ranging from 7.006 to 7.531. The arterial and the venous pCO2 ranged from 15.8 to 53.6 mm Hg and 16.5 to 44.9 mm Hg, respectively, whereas the arterial and venous bicarbonate levels ranged from 9.7 to 27.9 and 7.9 to 25.4 mmol/l, respectively.
The ICC for pH, pCO2 and bicarbonates was observed as 0.995, 0.929, and 0.946 (p-value = <0.001) respectively (Table 2, Figure 1). Moreover, the Bland–Altman method based on bias and 95% LOAs for arterial and venous measurements was used and the difference between them is shown in Figure 2. The bias plots showed statistically significant agreement in narrow acceptable ranges for all parameters except bicarbonates. The mean bias (SD, 95% LOA) was measured for pH 0.089 (SD = 0.00472, 95% LOA = 0.0181-0.0036); for pCO2 -1.1096 (SD = 1.0089, 95% LOA = 0.867-3.087) and for bicarbonate 1.124 (SD = 0.674, 95% LOA = 2.44-0.197). Low bias in the results thus indicated a strong agreement.
Discussion
The use of venous blood sample as a substituent for arterial sample for acid–base status determination has been evaluated in various diseases including diabetic ketoacidosis, acute respiratory failure, chronic obstructive pulmonary disease, cardiac arrest, and various other diseases.6,9,12,13 Medical literature continues to debate the usefulness of these laboratory findings in various diseases. Venous blood sample collection is relatively inexpensive and lesser laborious to collect and has been used for diagnosing and/or assessment of various diseases and for simultaneous determination of chemical or hematological parameters. Data regarding the usefulness of the VBG sample for septic patients presents with confounding results in the Asian population. Furthermore, there is no previous data on the efficacy of use of venous pH measurement in the local population of septic patients thus demanding an evaluation of their acid–base status. The current study may support the use of a potential sample (VBG) for acid–base status nevertheless the comparison and agreement of ABG and VBG in septic patients would need to be assessed in a larger Pakistani cohort.
Table 1. Demographic and clinical information of patients.
| Parameters | Subjects (n = 350) |
|---|---|
| Gender Male Female |
194 (55.4%) 156 (44.6%) |
| Age (Years) mean ± SD Adults (≥30-49 years) Male Female Elderly (≥50 years) Male Female Comorbidities Chronic heart failure Diabetes mellitus Chronic kidney disease Chronic obstructive pulmonary disease Smoking Hepatitis B & C |
48.06 ± 8.895 86 84 108 72 40 (11.4%) 72 (20.6%) 49 (14.0%) 52 (14.9%) 60 (17.1%) 77 (22%) |
*SD: Standard deviation.
Table 2. ICC and agreement between arterial and VBG measurements.
| Variable | ABG (n = 350) | VBG (n = 350) | ABG versus VBG Correlation | Bias | 95% LOA* |
|---|---|---|---|---|---|
| pH | 7.34 ± 0.96 | 7.32 ± 0.95 | 0.995 (<0.001) | 0.089 ± 0.00472 | 0.0181, 0.0036 |
| pCO2 (mm Hg) | 30.32 ± 5.38 | 32.54 ± 5.32 | 0.929 (<0.001) | -1.1096 ± 1.0089 | 0.867, 3.087 |
| Bicarbonate (mmol/l) | 19.32 ± 4.14 | 17.07 ± 3.84 | 0.946 (<0.001) | 1.124 ± 0.674 | 2.44, 0.197 |
*LOA: Limit of agreement.
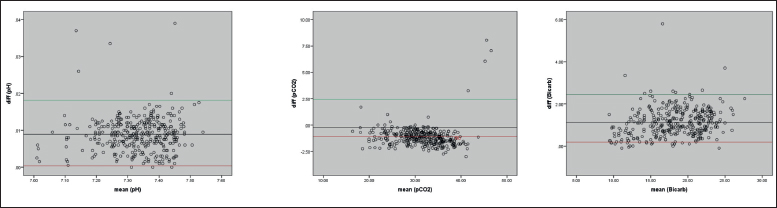
Figure 1. Scoring of NMP among 618 respondents (medical students).
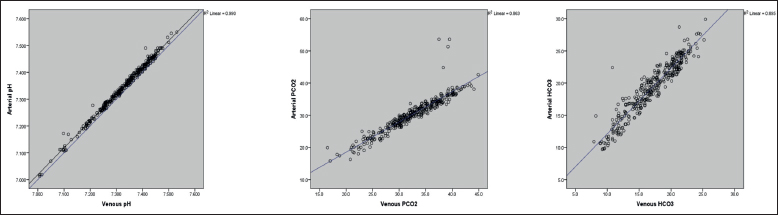
Figure 2. ICC between ABG and VBG for pH (left panel), pCO2 (middle panel), and bicarbonate (right panel).
The results of the present study depict that the ABG and VBG samples show interclass agreement for all three parameters i.e., pH, pCO2, and bicarbonate. When assessing the new tests, Altman and Bland suggested that agreement, not correlation, is significant.15 The bias plot (Bland–Altman) displays the difference between the tests against the estimation of the true result of the test (assumed to be the mean of the test results). Although the correlation was found significant for all the three variables, the Bland–Altman plots showed an agreement limited for pH and pCO2 only. Previous studies have reported that arterial pH is almost identical to venous pH.16 As shown in our results, a high agreement for pH value was observed (0.0181-0.0036, 95% LOA) which is notably better agreement as reported by Kelly et al.6 who reported an agreement range from -0.11 to 0.04 with 95% LOA. Our findings are also in a similar direction to the results reported by Middleton et al.16 where pH showed high agreement with a mean difference of 0.03 in ABG and VBG samples.
Similarly, the agreement in VBG and ABG for pCO2 has been demonstrated by previous studies in different pathological conditions. The study of Cuschieri et al.17 revealed an agreement in venous-arterial pCO2 differences and reported VBG as an alternate for calculating cardiac output. In the current study, agreement in VBG and ABG for pCO2 was also observed (0.867-3.087, 95% LOA) which is in line with the findings of Malinoski et al.,10 with 95% LOA. Contrary to the agreement of pH and pCO2, our findings for bicarbonate have shown a good correlation but exceed the 95% LOA. Although the previous studies have shown agreement for bicarbonate in ABG and VBG, our results indicated a slight increase from the limit of acceptance which might be due to ethnic differences and physiological variations or factors that exist in different ethnicities.9,10
Although there are no strict guidelines for assessing acid-base status in the management of sepsis, the pathophysiology of sepsis may reveal the usefulness of taking such an assessment regularly. Sepsis frequently leads to the development of acidosis, particularly when lactic acidosis and respiratory or renal failure occur. One can argue that determining the acid–base status should be a critical part of sepsis treatment and management. Since patients with sepsis typically have complex acid–base disorders, the use of VBG sample only for assessing the pH and pCO2 in the management of sepsis remains an open debate for the physicians. Furthermore, a logical interpretation should be incorporated in cases where clinical presentation does not match with the laboratory tests.
Conclusion
The VBG can be used as a substituent for ABG measurements for determining acid-base status in patients having sepsis and/or septic shock. An agreement exists between ABG and VBG for determination of pH and pCO2 in contrast to the bicarbonate levels.
Limitations of the Study
There are several limitations of our research work that should be taken into consideration while interpreting the results. The sample size was based on the expected mean difference of 0.80 in pCO2 with an expecting power of 81%. Further, the evidence generated from this study was based upon a sample cohort of the local population. Therefore, the results cannot be generalized to other ethnicities. To the best of our knowledge, the current study revealed an agreement of blood gas parameters taken from venous and arterial samples in septic shock patients for the first time in the local population and provide a baseline for future prospects. Moreover, further studies with a larger sample size and with detailed physical factors may contribute to validating our findings.
Acknowledgement
The authors would like to acknowledge the logistic and technical support given by the technical & non-technical staff of Medicine Department and Emergency Section of Jinnah hospital, Lahore, Pakistan.
List of Abbreviations
| ABG | Arterial blood gas |
| ICC | Interclass correlation |
| LOA | Limits of agreement |
| VBG | Venous blood gas |
Conflict of interest
None to declare.
Grant support and financial disclosure
None to disclose.
Ethical approval
Ethical approval for the study was obtained from the Institutional Review Board of Jinnah Hospital Lahore, Pakistan dated 08/07/2021 vide Letter No. (111/08/07/2021/S2ERB).
Author’s contributions
AP & KMK: Conception and design of the study, acquisition, interpretation of data, and drafting of the manuscript.
SB & ZG: Drafting of the manuscript and revising it critically for important intellectual content.
UP & XN: Sample collection, record keeping, statistical analysis and drafting of manuscript.
ALL AUTHORS: Approval of the final version of the manuscript to be published.
Authors’ Details
Abida Pervaiz1, Sadia Bashir2, Zareen Gulrohi3, Usman Pasha4, Xiao Ning5, Khalid Mehmud Khan1
- Senior Registrar, Department of Medicine, Jinnah Hospital Lahore, Lahore, Pakistan
- Medical Specialist, Department of Medicine, Tehsil Head Quarter Hospital, Wazirabad, Pakistan
- Senior Registrar, Department of Medicine, Avicenna Medical College & Hospital, Lahore, Pakistan
- PhD Scholar, School of Biochemistry & Biotechnology, University of the Punjab, Lahore, Pakistan
- Consultant Physician, Department of Medicine, Pakistan Kidney & Liver Institute and Research Centre (PKLI), Lahore, Pakistan
- Professor, Department of Medicine, Jinnah Hospital Lahore, Lahore, Pakistan
References
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29(7):1303–10. doi: 10.1097/00003246-200107000-00002
- Dickson S. Sepsis and multiple organ failure. Anaesth Intensive Care Med. 2009;10(4):165–8. doi.org/10.1016/j.mpaic.2009.01.008.
- Fleischmann C, Scherag A, Adhikari NK, Hartog CS, Tsaganos T, Schlattmann P, et al. Assessment of global incidence and mortality of hospital-treated sepsis. Current estimates and limitations. Am J Respir Crit Care Med. 2016;193(3):259–72. doi: 10.1164/rccm.201504-0781OC.
- Tiru B, DiNino EK, Orenstein A, Mailloux PT, Pesaturo A, Gupta A, et al. The economic and humanistic burden of severe sepsis. Pharmacoeconomics. 2015;33(9):925–37. doi: 10.1007/s40273-015-0282-y.
- Reinhart K, Daniels R, Kissoon N, Machado FR, Schachter RD, Finfer S. Recognizing sepsis as a global health priority—a WHO resolution. N Engl J Med. 2017;377(5):414–7. doi: 10.1056/NEJMp1707170.
- Kelly A-M, Kyle E, McAlpine R. Venous pCO2 and pH can be used to screen for significant hypercarbia in emergency patients with acute respiratory disease. J Emerg Med. 2002;22(1):15–9. doi: 10.1016/s0736-4679(01)00431-0.
- Rees SE, Hansen A, Toftegaard M, Pedersen J, Kristiensen SR, Harving H. Converting venous acid–base and oxygen status to arterial in patients with lung disease. Eur Respir J. 2009;33(5):1141–7. doi: 10.1183/09031936.00140408.
- Kelly AM, Klim S. Agreement between arterial and venous pH and pCO2 in patients undergoing non‐invasive ventilation in the emergency department. Emerg Med Australas. 2013;25(3):203–6. doi: 10.1111/1742-6723.12066.
- Ma OJ, Rush MD, Godfrey MM, Gaddis G. Arterial blood gas results rarely influence emergency physician management of patients with suspected diabetic ketoacidosis. Acad Emerg Med. 2003;10(8):836–41. DOI: 10.1111/j.1553-2712.2003.tb00625.x.
- Malinoski DJ, Todd SR, Slone DS, Mullins RJ, Schreiber MA. Correlation of central venous and arterial blood gas measurements in mechanically ventilated trauma patients. Arch Surg. 2005;140(11):1122–5. doi: 10.1001/archsurg.140.11.1122.
- McCanny P, Bennett K, Staunton P, McMahon G. Venous vs arterial blood gases in the assessment of patients presenting with an exacerbation of chronic obstructive pulmonary disease. Am J Emerg Med. 2012;30(6):896–900. doi: 10.1016/j.ajem.2011.06.011.
- McKeever TM, Hearson G, Housley G, Reynolds C, Kinnear W, Harrison TW, et al. Using venous blood gas analysis in the assessment of COPD exacerbations: a prospective cohort study. Thorax. 2016;71(3):210–5. doi: 10.1136/thoraxjnl-2015-207573.
- Steedman D, Robertson C. Acid base changes in arterial and central venous blood during cardiopulmonary resuscitation. Emerg Med J. 1992;9(2):169–76. doi: 10.1136/emj.9.2.169.
- Koul PA, Khan UH, Wani AA, Eachkoti R, Jan RA, Shah S, et al. Comparison and agreement between venous and arterial gas analysis in cardiopulmonary patients in Kashmir valley of the Indian subcontinent. Ann Thorac Med. 2011;6(1):33. doi: 10.4103/1817-1737.74274.
- Mansournia MA, Waters R, Nazemipour M, Bland M, Altman DG. Bland-Altman methods for comparing methods of measurement and response to criticisms. Glob Epidemiol. 2021;3:100045. doi.org/10.1016/j.gloepi.2020.100045
- Middleton P, Kelly A, Brown J, Robertson M. Agreement between arterial and central venous values for pH, bicarbonate, base excess, and lactate. Emerg Med. 2006;23(8):622–4. doi: 10.1136/emj.2006.035915
- Cuschieri J, Rivers EP, Donnino MW, Katilius M, Jacobsen G, Nguyen HB, et al. Central venous-arterial carbon dioxide difference as an indicator of cardiac index. Intensive Care Med. 2005;31(6):818–22. doi: 10.1007/s00134-005-2602-8.
- Schütz N, Roth D, Schwameis M, Röggla M, Domanovits H. Can venous blood gas be used as an alternative to arterial blood gas in intubated patients at admission to the emergency department? A retrospective study. Open Access Emerg Med. 2019:305–12. doi: 10.2147/OAEM.S228420
Keywords: Agreement, arterial blood gases, bias, sepsis, septic shock, venous blood gases

Publication History
Received: July 21, 2022
Revised: November 24, 2022
Accepted: December 13, 2022
Published: December 30, 2022
Authors
Sadia Bashir
Medical Specialist, Department of Medicine, Tehsil Head Quarter Hospital, Wazirabad, Pakistan.
Zareen Gulrohi
Senior Registrar, Department of Medicine, Avicenna Medical College & Hospital, Lahore, Pakistan.
Usman Pasha
Ph.D Scholar, School of Biochemistry & Biotechnology, University of the Punjab, Lahore, Pakistan.
Xiao Ning
Consultant Physician, Department of Medicine, Pakistan Kidney & Liver Institute and Research Centre (PKLI), Lahore, Pakistan.
Khalid Mehmud Khan
Professor, Department of Medicine, Jinnah Hospital Lahore, Pakistan.