Biomedica - Official Journal of University of Health Sciences, Lahore, Pakistan
Volume 37(3):134-138
OPINION
Integration among disciplines to integration into profession; a case for Integrated Discipline-Aligned (IDiAl) curriculum model for undergraduate medical education
Saima Chaudhry*
Received: 10 August 2021 Revised date: 01 September 2021 Accepted: 10 September 2021
Correspondence to: Saima Chaudhry
*PhD Scholar Medical Education, Head Department of Oral Pathology, University of Health Sciences, Lahore, Pakistan.
Email: saimachaudhry@uhs.edu.pk
Full list of author information is available at the end of the article.
ABSTRACT
Integration implies meaningful connections that can be applied to disciplines, domains, or linking education to real life practice. The essence of any integrated curriculum is a program that can improve patient care by graduating work ready professionals. Based on this approach, an Integrated Discipline-Aligned curriculum model is being proposed for undergraduate medical education in an effort to provide sound knowledge base with an explicit focus on clinical and professional skills so that doctors of tomorrow can meaningfully contribute to profession and society.
Keywords:
Curriculum, integration, medical education, undergraduate.
Medical subjects or disciplines in contemporary education have stood the test of time for over 100 years by training the best professional doctors around the globe. However, with advent of late 20th and early 21st century, there came an Internet revolution in the already existing information age. This resulted in change in the roles of the teacher and the student where later had to take responsibility of own learning while former had to start acting as a mentor, facilitator and a guide rather than a sole source of knowledge. Turn of the century also saw changes in the types, severity and pattern of diseases, the treatments evolved from general to personalized, health informatics, telehealth, and health security started gaining importance while evidence became more valued than expert opinion. Most importantly, access to information remained no more restricted to the professionals but reached the public who became more critical and demanding leading to different level of professional accountability for doctors who are now seen as normal human beings instead of someone possessing godly powers.
This phenomenon has called for a paradigm shift in the way learning experiences are planned for equipping medical students with 21st century skills to solve current and future health problems in a volatile, uncertain, complex and ambiguous world. Realizing this, World Federation for Medical Education, provided guidelines for undergraduate medical education to global accrediting bodies, calling on institutions to use and interpret the standards based on “own culture, resources, aspirations, and values, while still addressing the specified areas of performance.”1 These areas of performance are defined in terms of outcomes of a medical graduate, which with minor variations in terminology across countries, require tomorrow’s doctor to be skilful practitioner, professional and ethical, manager and leader, health advocate, scholar, communicator, collaborator, systems thinker, and life-long learner.
Current curriculum of Bachelor of Medicine & Bachelor of Surgery (MBBS) in Pakistan is hospital-based spanning over 5 years followed by 1 year of house job (clinical internship). In most of the cases, curriculum is discipline based with an annual system of assessment. There is a preclinical and clinical divide where hospital based clinical training of the students is started as part of formal curriculum in third year of medical college after 2 years of training in basic biomedical sciences. This curriculum provides strong foundation in basic concepts, processes and mechanisms of the disease resulting in graduates who are knowledgeable in medicine however, research highlights that this structure is not being able to equip medical graduates with required procedural skills, research acumen, empathy and professionalism, communication, collaboration and leadership skills that are mandatory for future doctors.2-4 This lack of ability is compounded by perceived sense of pride and superiority which is making doctors less tolerant of their colleagues within the health professions and less likely to seek help when required, resulting in lower level of performance, increased burnout and in turn, compromised patient care.5
This calls for a change in the way doctors are being trained in their undergraduate years with an emphasis on performance with an equal focus and meaningful connections between cognitive, psychomotor and affective domains of learning. Globally accrediting bodies are advocating incorporation of explicitly defined procedural skills, professionalism skills, research skills, leadership skills, collaborative and communication skills etc., in their curricula so that the teachers and those being taught clearly understand what is expected of them and at what level of performance.
Curricular structure considered most suitable for creating meaningful learning experiences that can help students make connections of their learning with the real world is generally referred to as “integrated curriculum.” The term gained popularity in medical education with the publication of Harden’s6 integration ladder, which builds on the integration models advocated for designing elementary school curriculum by Drake7, Jacobs8 and Fogarty.9 Curriculum designers generally have applied integration as a methodology to organize curricular elements under two main themes; horizontal integration and vertical integration. In horizontal integration cognitive scaffolding for students is ensured through a time table that has aligned teaching of similar concepts by all disciplines being taught within a year. In vertical integration the focus is creating coherence between foundational (biomedical and pathological) sciences and clinical sciences across years in an effort to contextualize all education and link it to practice. Term spiral integration is used in medical education literature when both horizontal and vertical integration exist in a curriculum.
Alongside integration another term that started gaining popularity is “modular.” In an effort to deepen connections among disciplines and between theoretical and practical knowledge, the disciplines started to be grouped under human organ systems. These study units are labelled as modules and the curriculum as modular which has been applied most often to foundational sciences (grouping subjects like Anatomy, Physiology and Biochemistry under the umbrella of organ systems like musculoskeletal or respiratory system), while the names of clinical science disciplines have stayed intact. Modules in essence are small study units that are independent of each other and in modular programs, students have a choice to study modules in their own chosen sequence of preference.10 This terminology is generally applied to non-linear programs which is not the case in MBBS where neither organ systems are completely independent of each other nor students choose the sequence of their studies. The literature highlights that modular curricula demand greater maturity on the part of the learner10 and it becomes challenging for students to understand the connections between disciplines without understanding the nature of disciplines. The change from discipline to module in foundational science teaching in undergraduate education has also forced the educators to decrease content of these disciplines which may result in medical graduates with a weak academic base.11
The regular combined use of terms “integration” and “modular” leads to misconception that a curriculum not based on modules cannot be labelled as integrated. This is debatable as integration has always been presented as a continuum, not as an all or nothing rule, in which the disciplines are identifiable till the level of transdisciplinary integration as highlighted by Sethi and Khan12 who grouped integration phenomenon into three systems; intradepartmental, interdepartmental and consolidation. Also Drake13 points out, “although teachers might organize transdisciplinary curriculum around a real-world context, the reality of covering the standards and grading in distinct subject areas quickly bring them back to disciplines.
All this discussion leads to one conclusion that this over emphasis on terminologies and jargons is making us myopic and shifting our focus from the essence of integration itself which is to improve patient care by graduating work ready doctors. It is the time for curriculum developers to change their approach and start visualizing integration not as a combination of subjects or organ systems, as units or modules or as an amalgamation of foundational and clinical sciences but, as highlighted by Wijnen-Meijer et al.14, “an educational approach that fosters a gradual increase of learner participation in the professional community through a stepwise increase of knowledge-based engagement in practice with graduated responsibilities in patient care.” This implies that if a curriculum strives to be integrated in true sense of the word, then after every year of training in medical school, students are able to carry out some professional tasks and responsibilities independently and feel “integrated” in the community of practice leading to persistent motivation, self-directed learning, and professional identity formation from the start of training to graduation and beyond.
With this philosophy of integration highlighted by all curricular reformers and realizing the shortcomings of half adopted modular system, a modified curricular model is being proposed for undergraduate medical education. This model is named Integrated Discipline-Aligned (IDiAl) curriculum in which subject (discipline) names are retained and these are grouped under larger themes. The four themes are: State of Health, State of Disease, Disease Prevention, and Disease Management (Figure 1). For making meaningful connections for learners’ disciplines are aligned under three categories: biomedical and preventive sciences (first 2 years), diagnostic sciences (third year), and clinical sciences (fourth and final year), which also align well with the major curriculum themes. This multidisciplinary structure with disciplinary aligned teaching will address the cognitive domain of learning by neither requiring a reduction in basic science content, thus not compromising factual knowledge base required to apply current learning to future disease processes, nor will cause any insecurity in faculty of foundational sciences.
Realizing the importance of explicitly defined skill set for contextualizing education and for meaningful transfer of knowledge to practice, this main framework is supported by two interdisciplinary spiral programs across 5 years; 1) Clinical skills in medicine (CSiM) addressing the procedural skills and thus the psychomotor domain of learning and 2) professionalism, ethics, research, and leadership skills (PERLS) spiral addressing the affective domain of learning. The domain specific objectives will be identified in line with the overall outcomes of doctors (Figure 2). All these domains will link through an aligned time table establishing meaningful connections within and across domains and study years.
The IDiAl curriculum model by providing sound knowledge base through disciplinary teaching and structured clinical and professional training through CSiM and PERLS programs, if implemented through sound principles of andragogy, envisions a humanistic doctor who will have the knowledge, skills and attitudes to be able to generate practice based evidence, advocate healthcare, counsel patients, collaborate within and outside the profession and lead healthcare teams and organizations to bring a sustainable change through continuous self and system improvement. The proposed model can also be used as a framework for designing curriculum of undergraduate programs of other health professions like dentistry, nursing and allied health sciences. IDiAl curricular model like all the other models is an effort to design a curriculum for health professionals that can “develop the ability to apply existing skills and knowledge in new ways in order to meet needs and solve problems as they arise.”15
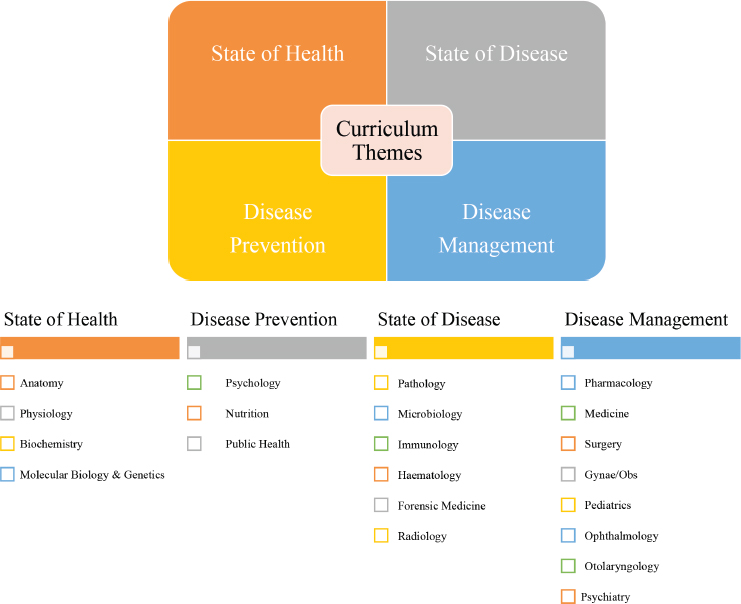
Figure 1. IDiAl curricular themes and proposed distribution of disciplines within themes.
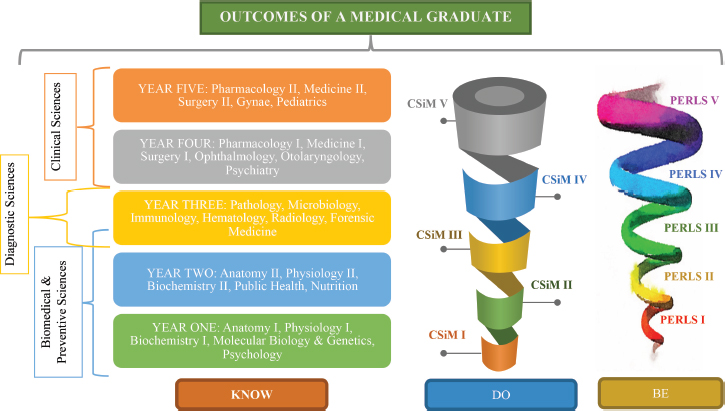
Figure 2. IDiAl curriculum model. Multidisciplinary curriculum structure with alignment among subjects along with two interdisciplinary spirals; CSiM (1-5) and PERLS (1-5) corresponding to academic years and addressing all learning domains derived from defined outcomes of a doctor.
List of Abbreviations
| CSiM | Clinical skills in medicine |
| IDiAL | Integrated discipline-aligned |
| PERLS | Professionalism, ethics, research, leadership skills |
Acknowledgement
All the curriculum reformers and designers and the colleagues who have helped me think critically regarding the topic.
Conflict of interest
None to declare.
Grant support and financial disclosure
None to disclose.
Ethical approval
Not applicable.
Author’s details
Saima Chaudhry1
Ph.D Scholar Medical Education, Head Department of Oral Pathology, University of Health Sciences, Lahore, Pakistan
References
- World Federation for Medical Education. Basic medical education. WFME global standards for quality improvement; 2020 [cited 2021 Aug]. Available from: https://wfme.org/wp-content/uploads/2020/12/WFME-BME-Standards-2020-1.pdf
- Bano U, Ahmed A, Tassadaq N. Medical professionalism: comparing views of public and doctors. PAFMJ. 2021;71(2):584–7. https://doi.org/10.51253/pafmj.v71i2.
4739 - Abbasi N, Çitaku F, Yasmeen R, Waldrop M, Khan YH, Zillioux D, et al. Identifying leadership competencies in medical and dental healthcare professionals in Pakistan. Open Access J Dent Sci. 2021;6(1):000290. https://doi.org/10.23880/oajds-16000290
- Jalil A, Zakar R, Zakar MZ, Fischer F. Patient satisfaction with doctor-patient interactions: a mixed methods study among diabetes mellitus patients in Pakistan. BMC Health Serv Res. 2017;17(1):155. https://doi.org/10.1186/s12913-017-2094-6
- Jalil A, Mahmood QK, Fischer F. Young medical doctors’ perspectives on professionalism: a qualitative study conducted in public hospitals in Pakistan. BMC Health Serv Res. 2020;20(1):847. https://doi.org/10.1186/s12913-020-05681-w
- Harden RM. The integration ladder: a tool for curriculum planning and evaluation. Med Educ. 2000;34(7):551–7. https://doi.org/10.1046/j.1365-2923.2000.00697.x
- Drake SM. Planning integrated curriculum: the call to adventure. Alexandria, VA: Association for Supervision and Curriculum Development; 1993 [cited 2020 Nov]. Available from: https://eric.ed.gov/?id=ED355660
- Jacobs HH. Interdisciplinary curriculum: design and implementation. Alexandria, VA: Association for Supervision and Curriculum Development; 1989 [cited 2021 Feb]. Available from: https://eric.ed.gov/?id=ED316506.
- Fogarty RJ. Ten ways to integrate curriculum. Educ Leadersh. 1991;49:61–5.
- Dejene W, Chen D. The practice of modularized curriculum in higher education institution: active learning and continuous assessment in focus. Cogent Educ. 2019;6(1):1611052. https://doi.org/10.1080/2331186X.2019.1611052
- Buja LM. Medical education today: all that glitters is not gold. BMC Med Educ. 2019;19(1):110. https://doi.org/10.1186/s12909-019-1535-9
- Sethi A, Khan RA. Curriculum integration: from ladder to ludo. Med Teach. 2020;42(12):1421–3. https://doi.org/10.1080/0142159X.2019.1707176
- Drake, Susan M. RCB. Meeting standards through integrated curriculum. Alexandria, VA: Association for Supervision and Curriculum Development; 2004 [cited 2020 Sep]. Available from: https://eric.ed.gov/?id=ED486683
- Wijnen-Meijer M, van den Broek S, Koens F, Ten Cate O. Vertical integration in medical education: the broader perspective. BMC Med Educ. 2020;20(1):509. https://doi.org/10.1186/s12909-020-02433-6
- Ontario, Ministry of Education and Training. The common curriculum: policies and outcomes. Grades 1–9. Ontario, Canada. The Ministry; 1995. pp 1–112.
Keywords: Curriculum, Integration, Medical Education, Undergraduate.

Publication History
Received: August 10, 2021
Revised: September 01, 2021
Accepted: September 10, 2021
Published: September 25, 2021
Authors
Saima Chaudhry
Assistant Professor, Department of Oral Pathology, University of Health Sciences, Lahore - Pakistan.