Original Article
Volume: 39 | Issue: 1 | Published: Mar 26, 2023 | Pages: 21 - 24 | DOI: 10.24911/BioMedica/5-802
Comparison of Single-Stage Reverse Sural Artery Flap Versus Two-Staged Interpolated Flap in Distal Lower Limb Injuries
Authors: Tauqeer Nazim , Sarfraz Ahmad , Kamran Hamid , Zahid Iqbal Bhatti , Muhammad Maaz Arif , Danish Mohsin
Article Info
Authors
Tauqeer Nazim
Assistant Professor, Department of Plastic Surgery, Sheikh Zayed Hospital, Lahore, Pakistan.
Sarfraz Ahmad
Associate Professor, Department of Plastic Surgery, Allama Iqbal Memorial Teaching Hospital, Sialkot, Pakistan.
Kamran Hamid
Senior Registrar, Department of General Surgery, Allama Iqbal Memorial Teaching Hospital, Sialkot, Pakistan.
Zahid Iqbal Bhatti
Assistant Professor, Department of Plastic Surgery, Nawaz Sharif Medical College, Gujrat, Pakistan.
Muhammad Maaz Arif
Lecturer, Department of Medical Education, University of Health Sciences, Lahore, Pakistan
Danish Mohsin
Assistant Registrar, Department of Medical Education, University of Health Sciences, Lahore, Pakistan.
Publication History
Received: October 25, 2022
Accepted: March 13, 2023
Published: March 26, 2023
Abstract
Background and Objective: Plastic surgeons face challenging conditions when dealing with soft tissue injuries or defects involving the lower part of the leg and the proximal part of the foot. The objective of the current study is to compare single-staged reverse sural artery flaps with two-staged interpolated flaps in distal lower limb injuries.
Methods: It was a prospective study carried out at the Department of Plastic Surgery, Allama Iqbal Memorial Teaching Hospital, Sialkot, Pakistan, over 5 years from 2015 to 2020. Sixty-eight (n = 68) patients with distal lower limb soft-tissue defects were enrolled and randomly allotted a two-stage interpolated flap design (group A) or single-stage reverse sural artery flap design (group B). The measured outcomes included the frequency of flap-tip necrosis, epidermolysis, partial or total flap loss, and additional procedures needed for managing these complications.
Results: Out of all the patients, 72% were of male gender and 28% were females with a mean age of 38.38 ± 10.76 years. In group A, there were 6% of the cases where tip necrosis was the only impediment as compared to 17% in group B. In patients of group A, epidermolysis was seen in 12% as compared to 35% in group B whereas only 6% of patients in group A required secondary procedures for flap tip necrosis as compared to group B (47%). Paired t-test was used to calculate the statistical significance of the outcome between the two groups (p-value of 0.0491).
Conclusion: The two-staged interpolated flap procedure results in fewer complications as compared to a single-staged reverse sural artery flap procedure. However, the shorter hospital stay in single-staged flap design is satisfying for the patients who did not report any complications with this procedure.
Keywords: Reverse flow, Flap, Superficial sural artery, Islandized, Interpolated

Biomedica - Official Journal of University of Health Sciences, Lahore, Pakistan
Volume 39(1):21-24
ORIGINAL ARTICLE
Comparison of single-stage reverse sural artery flap versus two-staged interpolated flap in distal lower limb injuries
Tauqeer Nazim1, Sarfraz Ahmad2, Kamran Hamid3, Zahid Iqbal Bhatti4, Muhammad Maaz Arif5*, Danish Mohsin6
Received: 25 October 2022 Revised date: 8 February 2023 Accepted: 13 March 2023
Correspondence to: Muhammad Maaz Arif
*Lecturer, Department of Medical Education, University of Health Sciences, Lahore, Pakistan.
Email: amerhassan@yahoo.com
Full list of author information is available at the end of the article.
ABSTRACT
Background and Objective:
Plastic surgeons face challenging conditions when dealing with soft tissue injuries or defects involving the lower part of the leg and the proximal part of the foot. The objective of the current study is to compare single-staged reverse sural artery flaps with two-staged interpolated flaps in distal lower limb injuries.
Methods:
It was a prospective study carried out at the Department of Plastic Surgery, Allama Iqbal Memorial Teaching Hospital, Sialkot, Pakistan, over 5 years from 2015 to 2020. Sixty-eight (n = 68) patients with distal lower limb soft-tissue defects were enrolled and randomly allotted a two-stage interpolated flap design (group A) or single-stage reverse sural artery flap design (group B). The measured outcomes included the frequency of flap-tip necrosis, epidermolysis, partial or total flap loss, and additional procedures needed for managing these complications.
Results:
Out of all the patients, 72% were of male gender and 28% were females with a mean age of 38.38 ± 10.76 years. In group A, there were 6% of the cases where tip necrosis was the only impediment as compared to 17% in group B. In patients of group A, epidermolysis was seen in 12% as compared to 35% in group B whereas only 6% of patients in group A required secondary procedures for flap tip necrosis as compared to group B (47%). Paired t-test was used to calculate the statistical significance of the outcome between the two groups (p-value of 0.0491).
Conclusion:
The two-staged interpolated flap procedure results in fewer complications as compared to a single-staged reverse sural artery flap procedure. However, the shorter hospital stay in single-staged flap design is satisfying for the patients who did not report any complications with this procedure.
Keywords:
Reverse flow superficial sural artery flap, single-staged flap, two-staged flap, interpolated flap, lower limb, soft tissue injuries.
Introduction
Providing soft tissue coverage in the distal lower limb is a significant challenge to surgeons. Such defects are not easily amenable to simple skin grafts as the lower limb region is more prone to ulcers, traumas, and vascular diseases due to a reduced arterial blood supply to this region. Although the cover is vital for vulnerable structures, microvascular surgical techniques using free flaps for these defects is another option but are both technically and economically demanding and cannot be done in remote areas with minimum infrastructure.1-3 The blood supply and anatomical distribution of vessels in the leg have made it possible to harvest large fascio-cutaneous flaps. Gaillard et al.4 described fascio-cutaneous flaps harvested over peroneal perforators. The dye injection studies carried out by Morris et al.,5 showed the pattern of these perforators and they also discussed the concept of “angiosome” to describe the network of vessels in a 3D pattern. This has allowed the harvesting of distal lower limb flaps based on neural structures and local perforators. Bulla et al.6 showed that the vascular network follows the superficial sensory nerve distribution. They evaluated the relationship between the arterial network of the posterior tibial artery perforators, the cutaneous nerves, and the superficial venous system in the lower third of the leg.
Hence reverse flow sural artery single-stage technique was studied to compare its outcomes with the two-stage interpolated flap in lower limb defects presenting in the local population.
Methods
This prospective study was conducted at the Plastic Surgery Department of Allama Iqbal Memorial Teaching Hospital, Sialkot, Pakistan over a period of 5 years (from March 2015 to July 2020). Sixty-eight (n = 68) patients with distal lower limb soft-tissue defects were included after taking the written informed consent. Ethical approval of the study was taken from the Plastic Surgery Department of Khawaja Muhammad Safdar Medical College, Sialkot, Pakistan.
Patients of either gender with isolated heel and ankle injuries requiring flap coverage were included in the study. Patients with a history of smoking or significant comorbid conditions like peripheral vascular diseases, bleeding disorders, diabetic foot ulcers, and venous ulcers or defects near the pivot point of the flaps were excluded.
A detailed history, complete physical examination, and investigations like complete blood profile and radiographic analysis were carried out in all patients. Patients were divided into two groups randomly via the lottery method; group A (n = 34) patients were surgically corrected with a two-stage interpolated flap design while group B (n = 34) patients were given single-stage reverse sural artery flap design surgical correction. Both groups were matched for age, gender, and size of the defect.
The two-stage technique involved raising the reverse sural flap along with a skin bridge or a paddle overlying the vascular pedicle and in the second stage, the bridge was divided and inset at the recipient site. The single-stage technique involved raising flaps overlying the vascular pedicle to skeletonize it and transfer it to the recipient site in the same operation. There was no need for pedicle division in the setting stage. All flap elevations were performed under a tourniquet in a prone position. The flap was marked by a line joining the mid popliteal point and midpoint between the lateral malleolus and tendoachilles. The flap’s pivot was marked at 5 cm above the lateral malleolus. Proximal one-fourth of the proximal leg was spared and the flap was centered over the longitudinal vascular axis. To raise a flap, an incision was given along the flap’s superior border. The vascular pedicle comprising the short saphenous vein, median superficial sural artery, and median cutaneous sural nerve were included within the flap. In all island flaps the skin covering the flap was undermined while in the interpolated flaps, the skin was harvested intact throughout its length. Around 3-4 cm wide subcutaneous fascial pedicle was retained to preserve vascularity. In the two-staged interpolated flap, the skin was kept intact over the pedicle, while in the one-staged flap, the skin incision was made all around the flap leaving a whole subcutaneous adipo-fascial pedicle. Then the harvested flap was maneuvered over the recipient’s defect as a subcutaneous tunnel of an interpolated flap. In the former group, if there was obvious pedicle compression, the skin bridge between the base of the flap and the defect was divided and the flap transposed without a subcutaneous tunnel. The raw area was covered with a split-thickness skin graft (STSG). The donor’s raw site was also covered with STSG if there was any remaining defect after primary closure. A plaster of Paris back slab was used to avoid compression on the pedicle. Postoperatively, flaps were followed for any signs of ischemia. To minimize the chances of post-op edema, patients were advised to lie in a prone position. Pedicle division and insetting were undertaken in the interpolated flaps after around a month under local anesthesia in adults. Full weight-bearing was permitted after 4 weeks of the first operation. The surgery on patients of each group was performed by the same experienced surgeon to maintain standardization. Data were collected by the principal investigator regarding the outcome of the patients.
Statistical analysis
Data were analyzed using Statistical Package for the Social Sciences (Version 22, Chicago, IL). Paired t-test was used to calculate the test of significance. The outcomes included hospital stay, flap survival, the frequency of complications in terms of flap tip necrosis, epidermolysis, and secondary procedures needed.
Results
There were 68 patients with 48 (72%) males and 20 (28%) females. The age ranged from 10 to 70 years with a mean age of 38.38 ± 10.76 years
The ulcer sites were hindfoot in (50%) n = 34 patients followed by ankles (15%) n = 10, heel (13%) n = 9, distal third of leg (10%) n = 7, and dorsum of proximal third of foot (12%) n = 8. The flap size ranged from 4 × 4 cm (16 cm2) to 11 × 15 cm (165 cm2) with a mean size of 60.11 ± 11 cm2. The hospital stay was 11-15 days with a mean of 12.22 ± 1.53 days in group A while it was 10-12 days with a mean of 9.71 ± 2.25 days in group B. In group A, there were 6% of the cases where tip necrosis was the only impediment as compared to 17% in group B. In patients of group A, epidermolysis was seen in 12% as compared to 35% in group B. A total of 6% of patients in group A required secondary procedures for flap tip necrosis as compared to group B (47%). Paired t-test was used to calculate statistical significance between the two groups and it showed a p-value of 0.0491 (Figure 1). Except in one case, the flap remained intact in all the patients and the average healing time was 18 days in all patients.
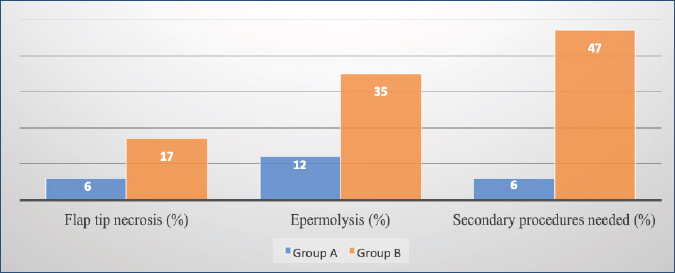
Figure 1. Complications in groups A and B indicated in terms of flap tip necrosis, epidermolysis, and secondary procedures needed.
Discussion
Complex soft tissue defects of the distal lower limb may be due to several different etiological factors. For example, trauma (wheel spoke injury), surgical procedures like tumor resection or burns, or due to trophic ulcers. This may result in exposed underlying structures like bones, joints, tendons, or prosthetic devices. For the majority of such defects, there remain two main reconstructive options; a free flap or a reverse flow superficial sural artery flap.3,7 The latter option was opted for in the present study due to the simplicity of the procedure and no requirement of microsurgery and also because it provides less bulky and pliable soft tissue coverage.7
The reverse flow superficial sural artery flap has a reliable and remarkably good blood supply at the ankle. Following vessels provide blood supply at this point: (i) fascio-cutaneous perforators, (ii) septo-cutaneous perforators, (iii) veno-cutaneous perforators, and (iv) neuro-cutaneous perforators.8 In studies done by Sarker et al.9 and Choi et al.,10 many patients had large soft tissue defects and for an alternative choice, a free flap would have sufficed. To avoid flap loss, they need to be rotated around 180° to cover the defect over the tendoachilles. De-epithelialized distal parts of the flap were used to fill the large soft tissue defects containing cavities. The donors required skin grafting to avoid deformity at the donor site.
The flap size as reported by Saaiq et al.11 ranged from 5 × 5 cm (25 cm2) to 15 × 15 cm (225 cm2) with a mean size of 82.11 ± 51.54 cm2 which is comparable to that of the present study. However, a higher number (76.47%) of patients in group B of Saaiq et al.11 required secondary procedures to address various flap-related complications in comparison to 47% patients of in group B in the present study. The hospital stay was 13-19 days (mean 14.61 ± 1.93 days) and 10 days, respectively, in patients who underwent reverse sural artery flap procedure as reported by Saaiq et al.11 and Thammannagowda et al.12
In the present study, although a single-stage sural artery flap was accompanied by higher flap tip necrosis and epidermolysis it was less cumbersome for a patient with a shorter hospital stay as compared to a two-stage interpolated flap. To reduce the incidence of partial necrosis Vendramin et al.13 from Brazil introduced a technique of leaving behind a minimum of 1.5 cm strip of skin over the adipo-fascial pedicle along with acquiring at least 1 cm extra fascio-subcutaneous margin beneath the flap’s skin portion. A two-stage procedure can be converted to a single-stage procedure by making an incision on the skin between the donor and recipient site as was done by Dhamangaonkar et al.14 This increases the rate of survival in flaps to 89.2% whereas skin edge necrosis was reported to be only 8.92% by Herlin et al.15
Conclusion
The two-staged interpolated flap procedure results in fewer complications as compared to a single-staged reverse sural artery flap procedure. However, the shorter hospital stay in single-staged flap design is satisfying for the patients who did not report any complications with this procedure. The results of the single staged flap are optimum with the least chances of flap loss despite being a complicated tissue defect.
Limitations of the Study
This study has been done on a small population hence results cannot be generalized to the whole population of Pakistan. Therefore, further studies in this field are encouraged by using large representative samples.
Acknowledgement
The authors are grateful to the Head of the Department of Plastic Surgery, Khawaja Muhammad Safdar Medical College, Sialkot, Pakistan for his help in carrying out this study. We are also thankful to Dr. Saira Khalid for her contribution to the article in terms of manuscript submission and guidance.
Conflict of interest
None to declare
Grant support and financial disclosure
None to disclose.
Ethical approval
The ethical approval was obtained from the Institutional Research Ethics Committee of Khawaja Muhammad Safdar Medical College, Sialkot, Pakistan vide letter no. 94/REC/KMSMC, dated 10-05-2022.
Authors’ contributions
TN, SA, KH, ZIB: Concept and design of the study, acquisition of data, and drafting of manuscript with intellectual input.
MA: Drafting of manuscript and intellectual input.
DM: Analysis of data and drafting of manuscript.
ALL AUTHORS: Approval of the final version of the maucript to be published.
Authors’ Details
Tauqeer Nazim1, Sarfraz Ahmad2, Kamran Hamid3, Zahid Iqbal Bhatti4, Muhammad Maaz Arif5, Danish Mohsin6
- Assistant Professor, Department of Plastic Surgery, Sheikh Zayed Hospital, Lahore, Pakistan
- Associate Professor, Department of Plastic Surgery, Allama Iqbal Memorial Teaching Hospital, Sialkot, Pakistan
- Senior Registrar, Department of General Surgery, Allama Iqbal Memorial Teaching Hospital, Sialkot, Pakistan
- Assistant Professor, Department of Plastic Surgery, Nawaz Sharif Medical College, Gujrat, Pakistan
- Lecturer, Department of Medical Education, University of Health Sciences, Lahore, Pakistan
- Assistant Registrar, Department of Medical Education, University of Health Sciences, Lahore, Pakistan
References
- Lachica RD. Evidence-based medicine: management of acute lower extremity trauma. Plast Reconstr Surg. 2017;139(1):287e–301e. https://doi.org/10.1097/PRS.0000000000002860
- Ebrahimi A, Nejadsarvari N, Ebrahimi A, Rasouli HR. Early reconstructions of complex lower extremity battlefield soft tissue wounds. World J Plast Surg. 2017;6(3):332–42.
- Pu LL. Free flaps in lower extremity reconstruction. Clin Plast Surg. 2021;48(2):201–14. https://doi.org/10.1016/j.cps.2020.12.002
- Gaillard J, Bourcheix LM, Masquelet AC. Perforators of the fibular artery and suprafascial network. Surg Radiol Anat. 2018;40(8):927–33. https://doi.org/10.1007/s00276-017-1927-7
- Morris SF, Tang M, Almutari K, Geddes C, Yang D. The anatomic basis of perforator flaps. Clin Plast Surg. 2010;37(4):553–70. https://doi.org/10.1016/j.cps.2010.06.006
- Bulla A, Bolletta A, Fiorot L, Maffei M, Bandiera P, Casoli V, et al. Posterior tibial perforators relationship with superficial nerves and veins: a cadaver study. Microsurgery. 2019;39(3):241–6. https://doi.org/10.1002/micr.30327
- Behan FC, Terrill PJ, Ashton MW. Fasciocutaneous island flaps for orthopaedic management in lower limb reconstruction using dermatomal precincts. Aust N Z J Surg. 1994;64(3):155–66. https://doi.org/10.1111/j.1445-2197.1994.tb02169.x
- Chowdhury MA, Khundkar SH, Ali MA, Islam MO. Soft tissue reconstruction around the ankle with sural artery flap. J Bangladesh Coll Phys Surg. 2018;36(3):101–6. https://doi.org/10.3329/jbcps.v36i3.37032
- Sarker A, Begum KN, Faruquee SR, Ali MA, Chowdhury MA, Manzur RM. Use of perforator propeller flaps for coverage of soft issue defects around the distal leg and ankle. J Bangladesh Coll Phys Surg. 2021;39(2):87–93. https://doi.org/10.3329/jbcps.v39i2.52388
- Choi JW, Kim YC, Oh TS, Koh KS, Jeong WS. The versatile use of revisited de-epithelialization concept in superficial circumflex iliac and anterolateral thigh perforator free flap for head and neck reconstructions. J Craniomaxillofac Surg. 2017;45(6):872–80. https://doi.org/10.1016/j.jcms.2017.02.010
- Saaiq M, Zimri FU. Reverse flow superficial sural artery fasciocutaneous flap: a comparison of outcome between interpolated flap design versus islanded flap design. World J Plast Surg. 2019;8(3):316–23.
- Thammannagowda, Ashish G, Mudukappa S, Pushkar D, Vijayakumar A. Comparison between peroneus brevis flap and reverse sural artery for coverage of lower one-third leg defects. ISRN Plast Surg. 2014(2014):969420 https://doi.org/10.1155/2014/969420
- Vendramin FS. Reverse-flow sural flap: 10 years of clinical experience and modifications. Rev Bras Cir Plást. 2012;27:309–15. https://doi.org/10.1590/S1983-51752012000200023
- Dhamangaonkar AC, Patankar HS. Reverse sural fasciocutaneous flap with a cutaneous pedicle to cover distal lower limb soft tissue defects: experience of 109 clinical cases. J Orthop Traumatol. 2014;15(3):225–9. https://doi.org/10.1007/s10195-014-0304-0
- Herlin C, Sinna R, Hamoui M, Canovas F, Captier G, Chaput B. Distal lower extremity coverage by distally based sural flaps: methods to increase their vascular reliability. Ann Chir Plast Esthet. 2017;62(1):45–54. https://doi.org/10.1016/j.anplas.2015.11.002