Case Report
Volume: 38 | Issue: 4 | Published: Dec 30, 2022 | Pages: 198 - 202 | DOI: 10.24911/BioMedica/5-843
Lipoma arborescence of knee joint in an adolescent male patient: a case report
Authors: Shuja Uddin , Adeel Hamid , Ahmed Umair Asad Khan , Hafiz M. Umar , Iqra Fatima , M. Rizwan Shah , Mian Muhammad Haneef
Article Info
Authors
Shuja Uddin
Lahore General Hospital, Lahore, Pakistan
Adeel Hamid
Assistant Professor, Department of Orthopedic Surgery, Lahore General Hospital, Lahore, Pakistan
Ahmed Umair Asad Khan
Postgraduate Resident, Department of Orthopedic Surgery, Lahore General Hospital, Lahore, Pakistan
Hafiz M. Umar
Consultant Orthopedic Surgeon, Tehsil Headquarter Hospital, Khanewal, Pakistan
Iqra Fatima
Postgraduate Resident, Radiology Department, Sir Ganga Ram Hospital, Lahore, Pakistan
M. Rizwan Shah
Assistant Professor, Department of Orthopedic Surgery, Lahore General Hospital, Lahore, Pakistan
Mian Muhammad Haneef
Professor, Department of Orthopedic Surgery, Lahore General Hospital, Lahore, Pakistan
Publication History
Received: September 24, 2022
Accepted: December 16, 2022
Published: December 30, 2022
Abstract
A very uncommon benign synovial membrane tumor is called lipoma arborescens. It often affects a single articulation, the knee. Despite a conventional imaging assessment, the lesion’s histological analysis is still required for the ultimate diagnosis. A 15-year-old boy attended the outpatient clinic of the Lahore General Hospital Lahore, Pakistan with pain and swelling in his left knee that had been steadily worsening over the previous 4 years. There were no concomitant prodromal symptoms, and the swelling was soft and non-tender while also inhibiting knee flexion. Soft tissue shadows were observed on radiographs. A large amount of subarticular erosion in the nearby tibial and femoral condyle was caused by the frond-like proliferation of fatty synovium, according to magnetic resonance imaging. Only the left knee joint showed focused areas of unusually elevated radionuclide uptake during the Technetium (Tc99m) bone scan. After an open synovectomy, the specimen underwent histological analysis, which revealed villiform fatty tissue, a hallmark of Lipoma arborescens coated by somewhat thicker synovium. Although infrequent, open synovectomy is currently the preferred course of treatment for lipoma arborescens, which should be taken into account when making a differential diagnosis of knee diseases. Approximately 3 months after surgery, the patient underwent his most recent follow-up and was asymptomatic with a small amount of joint effusion.
Keywords: Knee swelling, Lipoma arborescens, Synovectomy

Biomedica - Official Journal of University of Health Sciences, Lahore, Pakistan
Volume 38(4):198-202
CASE REPORT
Lipoma arborescence of knee joint in an adolescent male patient: a case report
Shuja Uddin1, Adeel Hamid2, Ahmed Umair Asad Khan3, Hafiz M. Umar4, Iqra Fatima5, Muhammad Rizwan Shah2, Mian Muhammad Haneef6
Received: 27 September 2022 Revised date: 08 November 2022 Accepted: 16 December 2022
Correspondence to: Shuja Uddin
*Consultant Orthopedic Surgeon, Department of Orthopedic Surgery, Lahore General Hospital, Lahore, Pakistan.
Email: Drshujauddin111@gmail.com
Full list of author information is available at the end of the article.
ABSTRACT
A very uncommon benign synovial membrane tumor is called lipoma arborescens. It often affects a single articulation, the knee. Despite a conventional imaging assessment, the lesion’s histological analysis is still required for the ultimate diagnosis. A 15-year-old boy attended the outpatient clinic of the Lahore General Hospital Lahore, Pakistan with pain and swelling in his left knee that had been steadily worsening over the previous 4 years. There were no concomitant prodromal symptoms, and the swelling was soft and non-tender while also inhibiting knee flexion. Soft tissue shadows were observed on radiographs. A large amount of subarticular erosion in the nearby tibial and femoral condyle was caused by the frond-like proliferation of fatty synovium, according to magnetic resonance imaging. Only the left knee joint showed focused areas of unusually elevated radionuclide uptake during the Technetium (Tc99m) bone scan. After an open synovectomy, the specimen underwent histological analysis, which revealed villiform fatty tissue, a hallmark of Lipoma arborescens coated by somewhat thicker synovium. Although infrequent, open synovectomy is currently the preferred course of treatment for lipoma arborescens, which should be taken into account when making a differential diagnosis of knee diseases. Approximately 3 months after surgery, the patient underwent his most recent follow-up and was asymptomatic with a small amount of joint effusion.
Keywords:
Knee, benign, tumor, lipoma arborescence, synovectomy.
Introduction
A rare, benign intra-articular lesion with an unidentifiable origin is called a lipoma arborescens (diffuse articular lipomatosis). It is distinguished by the synovium’s villous growth and the diffuse replacement of sub-synovial tissue by mature fat cells. The knee swelling, which is steadily increasing, is likely to be lipoma aborescence.1 The name “arborescens,” which refers to the distinctively tree-like morphology, is derived from the Latin word Arbour, which means “tree.” The most typical site of involvement is the knee, specifically over the supra-patellar zone, but other sites include the hip, wrist, and ankle.2 It is a rare form of intra-articular masses that emerges as a slowly increasing, painless swelling of the joint that lasts for years and is accompanied by sporadic effusions. We draw attention to this illness to acquire more knowledge of its clinical spectrum and diagnostic characteristics, allowing for an earlier detection, adequate intervention, and elimination of misdiagnosis as other, more difficult intra-articular masses.3 Although other joints can be compromised, the knee is typically involved, particularly at the suprapatellar pouch. Joint effusions or bleeding on occasion, varied discomfort, gradual joint swelling, and impaired range of motion are some symptoms. We also present a case of lipoma arborescens and on the basis of a literature review, describe the clinical characteristics, diagnosis, and management of this condition. Despite its rarity, patients with hemarthrosis or chronic joint swelling should have lipoma arborescens on their differential diagnosis list.4
Report of the Case
In July 2021, a 15-year-old boy, presented in the outdoor section of Lahore General Hospital, Lahore, Pakistan with complaints of insidious swelling and pain over the left knee joint, limiting the flexion of the knee, for the last 4 years. He denied that the joint had ever previously subluxed, dislocated, or locked. Over the years, swelling developed gradually along with mild to moderate pain. He had no prior experience with any injury or infection. He had treatment with non-steroidal anti-inflammatory medicines and underwent numerous examinations at various clinics. Arthrocentesis was performed under various conditions and resulted in the aspiration of clear fluid (Figure 1). Physical therapy assisted him in maintaining his range of motion and muscle function while tolerably reducing his symptoms. A painless soft palpable mass was found on the lateral aspect of the distal thigh during medical examination, along with a positive key sign indicating a moderate joint effusion, a reduction in range of motion with audible crepitus in the flexion-extension arc, and pain from patellofemoral joint compression. The mobility range was 0-100 degrees, with a 5-degree varus, although there was no sign of ligamentous laxity. Meniscal and ligament abnormalities were not detected by the particular test. Total leukocyte and differential cell counts were normal according to routine laboratory blood testing. There was no increase in the erythrocyte sedimentation rate. Other laboratory findings were unremarkable.
The MRI showed extensive subarticular erosion in the nearby tibial and femoral condyles, joint effusion, and thickening of synovial membranes with enhancement after contrast medium. Finger- or frond-like proliferation of fatty synovium was seen with the vast bulk of it lying on the lateral aspect of the joint (Figures 2 and 3). These frond-like growths in the synovium are more evident at the supra-patellar pouch and exhibit T1-hyperintense signals within the villi, which imply complete fat saturation. These observations validated lipoma arborescens.5 Following these investigations and fitness for anesthesia, an open synovectomy was performed (Figure 4), removing all the synovial lesions from the left knee joint and the sample was dispatched for histopathology. The morphology confirmed benign lipomatous tumor proliferating over the synovial tissue on microscopy.
Figure 1. Preoperatively, yellow-colored 2.0 ml aspirate collected from the knee joint in 5cc syringe.
Following the surgery, a drain suction was applied for 24 hours, collecting a volume of approximately 350 ml of blood on the second post-operative day. The physical therapy was commenced immediately after discharge, aiming to maintain the full range of motion and muscle control. Then the patient was allowed to support the weight on the affected limb as tolerated after 7 weeks of surgery. Thirty days after surgery, the patient was allowed to return to his usual activities. In his latest follow-up (approximately 3 months postoperatively), the patient was asymptomatic with minimal joint effusion.
Discussion
A rare form of benign synovial tumor is lipoma arborescence and the knee is the region in which it appears most frequently, followed by the shoulder, elbow, wrist, hip, and ankle.6 The majority of the time, it is unilateral; cases that are bilateral or that affect many joints are characterized as uncommon cases.7 It often strikes between the fourth and fifth decade of life, affecting both men and women in the same proportion. The oldest patient was 90 years old, and the youngest patient documented was 9 years old to date.8 As in this study, the patient’s age was 15 years and he presented with knee joint involvement. It is distinguished microscopically by adipocytes that have reached maturity substituting the synovial tissue, partially or completely. These tumors share many of the same clinical characteristics as other knee disorders, such as a continuous, gradual rise in joint volume without pain, and joint effusion.8 As the disease advances, the joint’s range of motion becomes restricted.9 The preferred examination is MRI. In a 9-year retrospective MR analysis of 6,387 knees at a hospital in Italy, only 9 cases were detected as lipoma arborescence, 7 cases with diffuse involvements, and 2 cases with nodular involvements but no synovial hypertrophy.10 It manifests as a synovial villous lump with an isointense fat signal.11 Free bone bodies, synovial chondromatosis, “rice bodies” (occurring in rheumatoid arthritis), pigmented villonodular synovitis, synovial hemangioma, intra-articular lipoma, and intra-articular liposarcoma are some of the conditions that necessitate differential diagnosis.12 This kind of tumor has not yet been shown to evolve into malignancy. Osteoarthritis of the afflicted joint is more likely to develop in patients who do not undergo thorough resection surgery at an early stage.8,11 The preferred way to proceed is an open synovectomy, then histopathology and following the surgery, recurrence is uncommon.12,13 There have been reports of video-arthroscopy and chemical synovectomy, however, the recurrence rate has been higher.12
In our case, we approached open synovectomy and the collected sample was sent for histopathological study for confirmation of diagnosis. The recovery period remained uneventful.
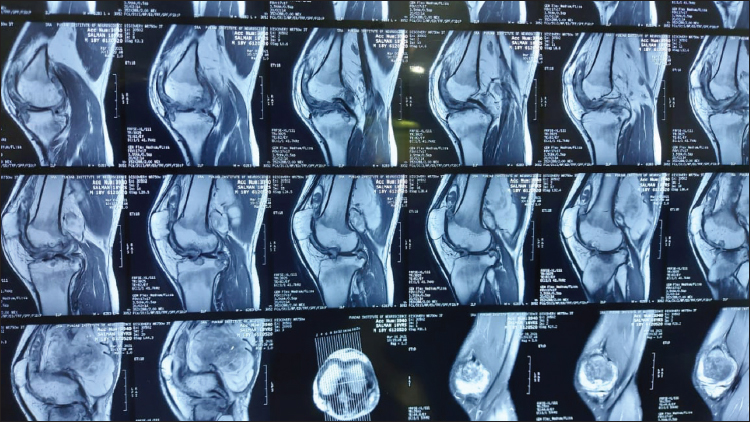
Figure 2. Magnetic resonance imaging (MRI) (sagittal) showing a delineated soft-tissue mass with high signal intensity with the subcutaneous fat. The tumor mass was occupying the patellofemoral space of the knee joint with extensive subarticular erosion in the nearby tibial and femoral condyles.
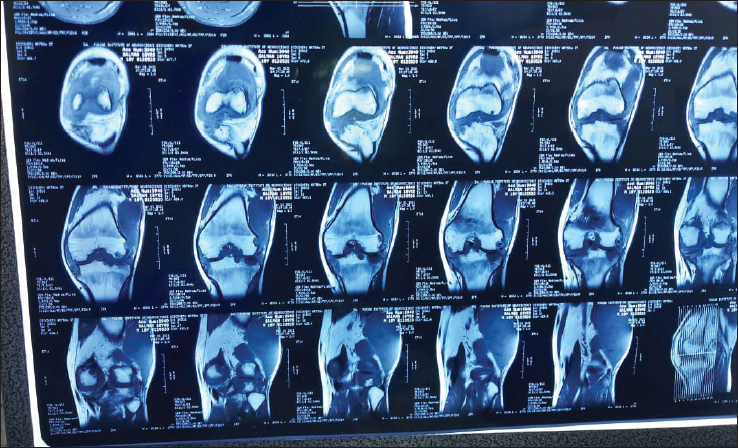
Figure 3. MRI (coronal) showing a lipomatous frond-like synovial mass with high signal intensity with the subcutaneous fat. The mass was occupying the patellofemoral space of the knee joint with a lateral predominance and mild effusion.
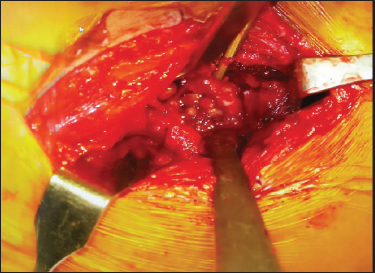
Figure 4. Per-operative image showing the presence of fronds like lipomatous mass occupying the knee joint.
Conclusion
A relatively uncommon benign primary intra-articular synovial tumor called lipoma arborescence presents with equivocal symptoms. The most crucial factor is a precise diagnosis made by clinical suspicion and imaging techniques. With complete resection, early and uneventful recovery can be achieved.
Acknowledgement
The authors would like to acknowledge the staff and residents of the Department of Orthopedic Surgery, Lahore General Hospital Lahore, Pakistan for their technical support during the surgical treatment and follow-up of this case.
List of Abbreviations
| MRI | magnetic resonance imaging |
Conflict of interest
None to declare.
Grant support and financial disclosure
None to disclose.
Ethical approval
As it is the case report, ethical approval was taken from the institute through the Professor and Head, Department of Orthopedic Surgery, Lahore General Hospital Lahore, Pakistan.
Authors’ contributions
SU, AUAK, MRS: Conception and design of study, acquisition, and analysis of data, drafting of the manuscript
HMU, IF, MMH: Acquisition of data, revision of manuscript with critical intellectual input.
ALL AUTHORS: Approval of the final version of the manuscript to be published.
Authors’ Details
Shuja Uddin1, Adeel Hamid2, Ahmed Umair Asad Khan3, Hafiz M. Umar4, Iqra Fatima5, M. Rizwan Shah2, Mian Muhammad Haneef6
- Consultant Orthopedic Surgeon, Department of Orthopedic Surgery, 1. Lahore General Hospital, Lahore, Pakistan
- Assistant Professor, Department of Orthopedic Surgery, Lahore General Hospital, Lahore, Pakistan
- Postgraduate Resident, Department of Orthopedic Surgery, Lahore General Hospital, Lahore, Pakistan
- Consultant Orthopedic Surgeon, Tehsil Headquarter Hospital, Khanewal, Pakistan
- Postgraduate Resident, Radiology Department, Sir Ganga Ram Hospital, Lahore, Pakistan
- Professor, Department of Orthopedic Surgery, Lahore General Hospital, Lahore, Pakistan
References
- Davies AP, Blewitt N. Lipoma arborescens of the knee. Knee. 2005;12(5):394–6. https://doi.org/10.1016/j.knee.2005.01.003
- Hallel T, Lew S, Bansal M. Villous lipomatous proliferation of the synovial membrane (lipoma arborescens). J Bone Joint Surg Am. 1988;70(2):264–70. https://doi.org/10.2106/00004623-198870020-00016
- Sanamandra SK, Ong KO. Lipoma arborescens. Singapore Med J. 2014;55(1):5–10. https://doi.org/10.11622/smedj.2014003
- Narváez J, Narváez JA, Ortega R, Juan-Mas A, Roig-Escofet D. Lipoma arborescens of the knee. Rev Rhum Engl Ed. 1999;66(6):351–3.
- Yan CH, Wong JWK, Yip DKH. Bilateral knee lipoma arborescens: a case report. J Orthop Surg. 2008;16(1):107–10. https://doi.org/10.1177/230949900801600125
- Tsifountoudis I, Kapoutsis D, Tzavellas A-N, Kalaitzoglou I, Tsikes A, Gkouvas G. Lipoma arborescens of the knee: report of three cases and review of the literature. Case Rep Med. 2017;2017:3569512. https://doi.org/10.1155/2017/3569512
- Siva C, Brasington R, Totty W, Sotelo A, Atkinson J. Synovial lipomatosis (lipoma arborescens) affecting multiple joints in a patient with congenital short bowel syndrome. J Rheumatol. 2002;29(5):1088–92
- Johandi F, Chua Z, Malhotra R, Wang W. Knee pain: a cautionary tale of lipoma arborescens. BMJ Case Rep. 2016;2016:bcr2015214049. https://doi.org/10.1136/bcr-2015-214049
- Kamran F, Kavin K, Vijay S, Shivanand G. Bilateral lipoma arborescens with osteoarthritis knee: case report and literature review. J Clin Orthop Trauma. 2015;6(2):131–6. https://doi.org/10.1016/j.jcot.2014.12.006
- Lovane A, Sorrentino F, Pace L, Galia M, Nicosia A, Midiri M, et al. Findings in lipoma arborescens of the knee: our experience. Radiol Med. 2005;109(5-6):540–6
- Cerqueira WS, Melo RAB de, Costa FD, Comunello J, Bitencourt AGV, Chung WT. Lipoma arborescens of the elbow: a case with features of a high-grade tumor. Rev Bras Ortop. 2018;53(2):252–6. https://doi.org/10.1016/j.rbo.2017.03.002
- Patil PB, Kamalapur MG, Joshi SK, Dasar SK, Rao RV. Lipoma arborescens of knee joint: role of imaging. J Radiol Case Rep. 2011;5(11):17–25. https://doi.org/10.3941/jrcr.v5i11.783
- Spaans AJ, Turkenburg JL, Wagenmakers R. Lipoma arborescens: an unusual cause of swelling of the knee. Radiol Case Rep. 2013;8(1):793. https://doi.org/10.2484/rcr.v8i1.793