Original Article
Volume: 38 | Issue: 4 | Published: Dec 30, 2022 | Pages: 214 - 218 | DOI: 10.24911/BioMedica/5-876
Serum calcium levels as biomarkers of birth asphyxia in neonates
Authors: Maria Hassan , Iffat Batool , Hasan Mujtaba , Muhammad Mohsin Javaid
Article Info
Authors
Maria Hassan
Consultant Pediatrician, THQ Hospital Gujar Khan, Primary & Secondary Health Department, Govt. of Punjab, Rawalpindi, Pakistan.
Iffat Batool
Assistant Professor, Department of Pediatrics, Fauji Foundation University, School of Health Sciences, Islamabad, Pakistan.
Hasan Mujtaba
Associate Professor, Department of Pathology, Shaheed Zulfiqar Ali Bhutto Medical University, Islamabad, Pakistan.
Muhammad Mohsin Javaid
PhD Scholar, Health Services Academy, Islamabad, Pakistan.
Publication History
Received: September 03, 2022
Accepted: December 18, 2022
Published: December 30, 2022
Abstract
Background and objective: Birth asphyxia is a common pathological condition seen in newborns with increased morbidity and mortality. Grave consequences following birth asphyxia require earlier recognition of the precipitating factors and prompt treatment in intensive care units. Multiple electrolyte imbalance has been related to this condition. This study aimed at determining the mean serum total calcium levels in neonates with birth asphyxia.
Methods: This cross sectional study was performed at the neonatal intensive care unit of the Pediatric Department of Fauji Foundation Hospital, Rawalpindi, Pakistan over a period of 6 months. A total of 100 full-term neonates of either gender with evidence of birth asphyxia of any stage were enrolled on their first hour of birth. Serum calcium levels were estimated in each neonate at 24 hours after birth.
Results: A total of 60 (60%) neonates were males. Mean serum calcium levels were found to be 7.64 mg/dl ± 0.59 with no significant difference among males and females (7.67 ± 0.64 and 7.59 ± 0.50 mg/dl, respectively). Neonatal distribution in Stages I, II, and III was 64 (64.0%), 23 (23.0%), and 13 (13.0%), respectively. Hypoxic-ischemic encephalopathy stage stratification with mean serum calcium levels with higher stages deciphered significant correlation (7.89 ± 0.54, 7.36 ± 0.28, and 6.88 ± 0.28 mg/dl, respectively, in stage I, II, and III).
Conclusion: Markedly decreased levels of mean serum calcium were seen in higher hypoxic stages with ischemic encephalopathy hence delineating a linear correlation with the onset and progression of disease.
Keywords: Birth asphyxia, hypocalcemia, hypoxic-ischemic encephalopathy, neonates, serum calcium

Biomedica - Official Journal of University of Health Sciences, Lahore, Pakistan
Volume 38(4):214-218
ORIGINAL ARTICLE
Serum calcium levels as biomarkers of birth asphyxia in neonates
Maria Hassan1, Iffat Batool2, Hasan Mujtaba3*, Muhammad Mohsin Javaid4,5
Received: 3 September 2022 Revised date: 10 November 2022 Accepted: 18 December 2022
Correspondence to: Hasan Mujtaba
*Associate Professor, Department of Pathology, Shaheed Zulfiqar Ali Bhutto Medical University, Islamabad, Pakistan.
Email: h_mujtaba@outlook.com
Full list of author information is available at the end of the article.
ABSTRACT
Background and objective:
Birth asphyxia is a common pathological condition seen in newborns with increased morbidity and mortality. Grave consequences following birth asphyxia require earlier recognition of the precipitating factors and prompt treatment in intensive care units. Multiple electrolyte imbalance has been related to this condition. This study aimed at determining the mean serum total calcium levels in neonates with birth asphyxia.
Methods:
This cross sectional study was performed at the neonatal intensive care unit of the Pediatric Department of Fauji Foundation Hospital, Rawalpindi, Pakistan over a period of 6 months. A total of 100 full-term neonates of either gender with evidence of birth asphyxia of any stage were enrolled on their first hour of birth. Serum calcium levels were estimated in each neonate at 24 hours after birth.
Results:
A total of 60 (60%) neonates were males. Mean serum calcium levels were found to be 7.64 mg/dl ± 0.59 with no significant difference among males and females (7.67 ± 0.٦٤ and ٧.5٩ ± 0.50 mg/dl, respectively). Neonatal distribution in Stages I, II, and III was 64 (64.0%), 23 (23.0%), and 13 (13.0%), respectively. Hypoxic-ischemic encephalopathy stage stratification with mean serum calcium levels with higher stages deciphered significant correlation (7.89 ± 0.54, 7.36 ± 0.28, and 6.88 ± 0.28 mg/dl, respectively, in stage I, II, and III).
Conclusion:
Markedly decreased levels of mean serum calcium were seen in higher hypoxic stages with ischemic encephalopathy hence delineating a linear correlation with the onset and progression of disease.
Keywords:
Birth asphyxia, neonates, hypocalcemia, seru calcium, hypoxic-ischemic encephalopathy.
Introduction
According to the definition of World Health Organization, birth asphyxia is a failure in the ability to initiate or sustain the process of breathing at the time of birth.1 Several metabolic derangements are observed in cases of birth asphyxia including calcium, sodium, potassium, phosphate, and glucose. A total of 130 billion babies are born each year out of which 4 million die in their neonatal period. Most of these deaths are reported from countries that have middle or low income with a reported overall 23% prevalence of birth asphyxia in such cases. Imbalance of electrolytes has been found to be associated with hypoxia inducedencephalopathy leading to increased morbidity and mortality.2,3 Consequently, multi-organ failure and electrolyte imbalance has been linked as a major reason for intensive care admissions. At the cellular level, adequate supply of oxygen is necessary for metabolism. Hypoxia, hypercarbia, and acidosis, which are seen in asphyxiated newborns, can lead to detrimental effects which necessitate prompt detection and treatment of the cause.4,5 An estimated 1 million children escaping birth asphyxia develop other central nervous system pathologies including neuromuscular, cognitive, and learning difficulties. Lack of oxygen due to inability to breathe can cause a decrease in oxygen supply to the brain causing hypoxic ischemic encephalopathy (HIE).6 Levels of several markers like brain-specific creatinine kinase, lactate dehydrogenase, lactate/creatinine ratio, glial fibrillary acidic protein, uric acid, hypoxanthine, glutamate, etc. in the blood or cerebrospinal fluid are used to determine brain injury.7 In birth asphyxia, overstimulation of neurotransmitter receptors results in a raised intracellular calcium, with subsequent destructive process. Calcium is a vital second messenger system hence helps in muscle function and acts as a cofactor for many enzymes. It is actively transported across the placenta in the third trimester leading to hypercalcemia in a term newborn (10-11 mg/dl) followed by abrupt recession due to cessation of maternal calcium resulting in hypocalcemia at 24 hours of life (8-9 mg/dl) and then normal levels are achieved by the second week.8 Literature elucidated a significant negative and positive correlation of serum potassium and calcium levels, respectively, with Apgar score. Magnesium has a significant role in preventing cell death in asphyxia.9,10 The importance of glucose in the body is just like fuel to the vehicles and inadequacy of glucose in newborns lead to prolonged neurological injuries as it is the main ingredient in aerobic metabolism at the cellular level.11 Birth asphyxia involves a cascade of events which effect multiple organs and the existing literature has found positive significant correlation between serum calcium and hypoxic injury. Newborns with severe hypoxic injury to the brain had decreased levels of calcium signifying the severity of HIE.12
This study aims to determine the serum total calcium levels as a predictor of advanced hypoxic stages in neonates with birth asphyxia born at a local tertiary care hospital of Pakistan.
Methods
This cross sectional descriptive study was conducted at the NICU, Pediatric Department, Fauji Foundation Hospital, Rawalpindi, Pakistan over 6 months period (October 2020 to April 2021) after approval of the Institutional Ethical Review Committee.
The calculated sample size for the study was (100) with the population mean of 7.00 ± 0.69 (d: 0.3) at a 95% confidence level and 5% margin of error.11 Written informed consent was obtained from the parents and confidentiality was maintained for inclusion in the study according to the guidelines of the Helsinki Declaration. Full-term neonates of both genders (completed 37 weeks of gestation) with evidence of birth asphyxia (any stage) were included. However, neonates with evidence of sepsis, infections, and major congenital pathologies were excluded.
All appropriate entries were recorded on predesigned proforma regarding age, gender, birth weight, and stage of HIE12 (Table 1) by a senior consultant. Serum calcium levels were estimated at 24 hours after birth. Using an aseptic technique, 3 ml of blood was obtained by venipuncture at 24 hours of life in a clean sterilized vial and transported to the chemical laboratory where serum was separated using a pipette and centrifuged at 3,000-4,000 rpm for 5-10 minutes with analysis on the same day. Serum total calcium levels were then measured using a direct colorimetric complexometric test (Arsenazo III) endpoint. Equation of the reaction was “Calcium+Arsenzo-III {2,7-[bis(2-arsonophenylazo)]-1,8-dihydroxy naphthalene-3,6-disulphonic acid} - Blue colored Complex.” The color intensity was directly proportional to the serum total calcium concentration. The pathologist verified the report and results were recorded.
Table 1. Sarnat staging of neonatal hypoxic-ischemic encephalopathy.13
| Stage | Symptoms |
|---|---|
| Mild | Irritable/hyperalert, the tone is normal/increased, tendon reflexes are brisk, seizures are absent and complex reflexes are normal. |
| Moderate | Lethargic, hypotonic, tendon reflexes are brisk, seizures are frequent and complex reflexes are weak. |
| Severe | Comatose, flaccid, tendon reflexes are depressed/absent, seizures are absent and complex reflexes are absent. |
Statistical analysis
Data entry and analysis were done using data management software IBM SPSS (version 23.0). Analysis of qualitative variables was done by calculating frequencies and percentages like gender and stage of HIE while the mean and standard deviation was calculated for quantitative variables like age, serum total calcium levels. An independent sample t-test was applied. A p-value of ≤0.05 was considered statistically significant.
Results
Total 100 patients who were full-term neonates of either gender with evidence of birth asphyxia of any stage were enrolled on their first hour of birth. A total of 60 (60%) were males whereas 40 (40%) were females. Mean serum calcium levels were found to be 7.64 ± 0.59 mg/dl in the study population. Difference in the mean serum calcium levels among males and females was not significant (7.67 ± 0.64 and 7.59 ± 0.50 mg/dl, respectively; p = 0.219). Neonatal distribution in Stage I, II, and III was 64 (64.0%), 23 (23.0%), and 13 (13.0%), respectively. Stratification concerning the HIE stage showed a significant correlation (p = 0.001) with mean serum calcium levels (7.89 ± 0.54, 7.36 ± 0.28, and 6.88 ± 0.28 mg/dl respectively in stages I, II, and III) (Tables 2 and 3). Mean serum calcium levels and HIE stages are shown in Figure 1.
Discussion
Perinatal asphyxia is a frequent and crucial medical issue in the management of labor and delivery. Andrew et al.11 enrolled 75 newborns of which 50 suffered from asphyxia. Serum calcium levels were recorded at the age of 24, 72, and 120 hours and results concluded severe decreased levels of calcium in the blood for birth till the fifth day of life.Numerous metabolic derangements exist in asphyxiated newborns such as hypoglycemia, hypocalcemia, hypomagnesemia, etc.12 In the present study, the levels of calcium in the blood were decreased significantly in newborns who had birth asphyxia and such decrease was directly proportional to the severity of birth asphyxia. These results are consistent with Manzke and Kruse14 who concluded that both the total and ionized calcium levels in asphyxiated newborns were decreased as compared to the ones who were born healthy.
Jajoo et al.15 studied the impact of serum calcium and phosphorus on asphyxiated newborns. Serial measurements of these electrolytes in the blood from birth till the fifth day of life revealed that babies born with birth asphyxia had low levels of calcium and phosphorous. In comparison, these electrolytes were found within the normal limits in healthy newborns. They concluded that lack of calcium and phosphorous intake may lead to a pathological condition resulting in asphyxia in newborns which can increase the morbidity and mortality in newborns.
Table 2. Correlation of mean serum calcium levels and HIE (Stage I and Stage III).
| HIE stage | N (%) | Mean calcium levels (mg/dl) | p-value |
|---|---|---|---|
| Stage I | 64 (64%) | 7.89 ± 0.54 | 0.001* |
| Stage III | 13 (13%) | 6.88 ± 0.28 |
*Significant p-value.
Table 3. Correlation of mean serum calcium levels and HIE (Stage II and Stage III).
| HIE stage | N (%) | Mean calcium levels (mg/dl) | p-value |
|---|---|---|---|
| Stage II | 23 (23%) | 7.36 ± 0.28 | 0.001* |
| Stage III | 13 (13%) | 6.88 ± 0.28 |
*Significant p-value.
According to a study conducted by Schedewie et al.,16 asphyxiated infants exhibited significantly low plasma calcium concentrations than their controls. Pyati et al.,10 in their research correlated the levels of electrolytes in the blood and the severity of birth asphyxia. Serum levels of calcium (6.85 ± 0.95 vs. 9.50 ± 0.51 mg/dl; p-value 0.001) and sodium (122.1 ± 6.0 vs. 138.8 ± 2.7 m Eq/l; p-value < 0.05) were significantly lower in cases versus controls (healthy newborns) while serum potassium levels were higher (5.05 ± 0.63 vs. 4.19 ± 0.40 m Eq/l; p-value 0.05).10 Among asphyxiated newborn patients, significant hypocalcemia and hyponatremia showed a positive linear correlation with the low levels of APGAR score while a negative linear correlation was found between APGAR scores and serum potassium levels.17 Saha et al.,18 in their case-control study aimed to find a correlation between birth asphyxia and serum levels of glucose, calcium and magnesium. Total 60 neonates were included in the study with 30 patients each in 2 groups of asphyxiated and healthy newborns who were less than 24 hours of age. Newborns with asphyxia (cases) and healthy newborns (controls) showed significant variations in the mean serum levels of calcium and values of serum calcium (7.37 ± 0.10 vs. 8.04 ± 0.09 mg/dl).18
Rai et al.19 performed a similar study to find how asphyxia can affect the levels of glucose and calcium in the blood. It was found that the asphyxia became more severe with the severity relating significantly with the decreased calcium and glucose levels in the blood.1 It is suggested that pathophysiology of asphyxia is due to oxidative stress in the mitochondria and dysregulation of calcium signaling at the molecular level.20 The progress of the disease is extremely complex and includes obstetric, gestational, and fetal risk factors.21 It is reported that the severity of HIE also directly correlates with the serum electrolytes, mainly calcium, sodium and potassium.22 Behrman et al.23 enrolled 42 infants with birth asphyxia (1-minute Apgar Score of 6 or less), and 42 control infants with equivalent gestational age and studied them serially from birth to 72 hours of age. In infants with birth asphyxia, serum calcium at 12 and 24 hours was lower than that of control infants and serum magnesium was lower from 12 to 48 hours. No differences were detected in urinary calcium and magnesium excretion.23 Lower serum calcium values were found in asphyxiated infants who received sodium bicarbonate therapy, even when gestational age was considered. Authors concluded that that bicarbonate therapy, increased phosphate loads, and functional hypoparathyroidism may play contributory roles in the pathogenesis of the hypocalcemia of birth asphyxia.24
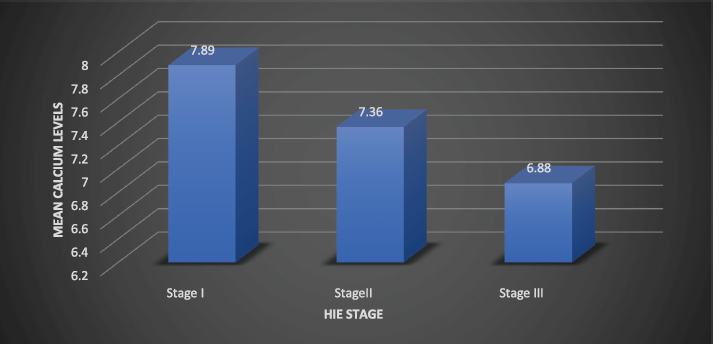
Figure 1. Mean serum calcium levels and HIE stage.
This study also highlights the significance and clinical impact of biochemical parameters in birth asphyxiated neonates and their association with the severity of HIE in our population as this would help the neonatologists in the early initiation of curative management.
Conclusion
Mean serum calcium levels show a linear correlation with the birth asphyxia and advanced stages of hypoxic-ischemic encephalopathy in neonates.
Limitations
Limitations of this study include that only calcium levels were monitored with respect to asphyxia. As asphyxia is multifactorial but calcium levels are the main contributing electrolyte. Further studies with better research design and evaluation of associated electrolytes should be conducted on a larger sample size.
List of Abbreviations
| HIE | Hypoxic-ischemic encephalopathy |
Conflict of interest
None to declare.
Grant support and financial disclosure
None to disclose.
Ethical approval
The study was conducted after approval of the Institutional Ethical Review Committee of the Fauji Foundation Hospital, Rawalpindi vide Letetr No. RTMC-S-122-132 dated 16th November, 2019
Authors’ contributions
MH: Conception and design of study, acquisition of data, drafting of manuscript with critical intellectual input.
IB: Acquisition and analysis of data, drafting of manuscript
HM: Critically revised the manuscript with intellectual input
MJ: Acquisition of data, drafting of manuscript.
ALL AUTHORS: Approval of the final version of the manuscript to be published
Authors’ Details
Maria Hassan1, Iffat Batool2, Hasan Mujtaba3, Muhammad Mohsin Javaid4
- Consultant Pediatrician, THQ Hospital Gujar Khan, Primary & Secondary Health Department, Govt. of Punjab, Rawalpindi, Pakistan
- Assistant Professor, Department of Pediatrics, Fauji Foundation University, School of Health Sciences, Islamabad, Pakistan
- Associate Professor, Department of Pathology, Shaheed Zulfiqar Ali Bhutto Medical University, Islamabad, Pakistan
- PhD Scholar, Health Services Academy, Islamabad, Pakistan
- Demonstrator, Department of Community and Preventive Dentistry, Shaheed Zulfiqar Ali Bhutto Medical University, Islamabad, Pakistan
References
- Lawn JE, Blencowe H, Waiswa P, Amouzou A, Mathers C, Hogan D, et al. Ending preventable stillbirths series study group; lancet stillbirth epidemiology investigator group. Stillbirths: rates, risk factors, and acceleration towards 2030. Lancet. 2016;387(10018):587–603. doi: 10.1016/S0140-6736(15)00837-5.
- Thakur J, Bhatta NK, Singh RR, Poudel P, Lamsal M, Shakya A. Prevalence of electrolyte disturbances in perinatal asphyxia: a prospective study. Ital J Pediatr. 2018;44(1):1–6. doi: 10.1186/s13052-018-0496-7.
- Acharya A, Swain B, Pradhan S, Jena PK, Mohakud NK, Swain A, et al. Clinico-biochemical correlation in birth asphyxia and its effects on outcome. Cureus. 2020;12(11):e11407. doi: 10.7759/cureus.
- Singh BB, Chandwani C, Mahajan K, Singh G. Total serum calcium and ionic calcium levels in birth Asphyxia: a prospective study. J Clin Diagn Res. 2020;14(3). doi: 10.7860/jcdr/2020/43363.13594.
- Bahatkar K, Aundhakar CD. Electrolyte status and plasma glucose levels in birth asphyxia: a case-control study. J Med Sci. 2021;41(1):17. doi: 10.4103/jmedsci.jmedsci_93_20.
- Odo KE, Odetunde OI, Chinawa JM, Okafor HU, Aronu AE, Adimora GN. Comparison of plasma electrolytes of perinatally asphyxiated and normal term babies. J Neonatal Perinat Med. 2019;12(4):385–9. doi: 10.3233/NPM-1839.
- Karlo J, Bhat BV, Koner BC, Adhisivam B. Evaluation of renal function in term babies with perinatal asphyxia. Indian J Pediatr. 2014;81(3):243–7. doi: 10.1007/s12098-013-1068-x.
- Zhang Y, Zeng HH. Renal function profiles in preterm neonates with birth asphyxia within the first 24 H of life. Front Pediatr. 2020;8:583–40. doi: 10.3389/fped.2020.583540.
- Mahajan K, Singh BB, Chandwani C, Singh V. Correlation of total serum calcium and ionic calcium levels with severity of birth Asphyxia. Indian J Public Health. 2020;11(03):503.
- Pyati AK, Khanikekar PK, Shetkar NR, Patil MM, Jaju PB, Karra ML, et al. Association of cord blood glucose, sodium, potassium, and calcium levels with neonatal birth asphyxia: a hospital-based study. Cureus. 2022;14(6). doi: 10.7759/cureus.261155.
- Andrew RD, Hartings JA, Ayata C, Brennan KC, Dawson-Scully KD, Farkas E, et al. The critical role of spreading depolarizations in early brain injury: consensus and contention. Neurocritical Care. 2022;37(Suppl 1):83–101.
- Zaman R, Mollah AH, Chowdhury MMR, Yeasmin S, Chowdhury AS, Saha D. Serum magnesium and calcium status among term asphyxiated newborns with moderate to severe hypoxic-ischemic encephalopathy (HIE). J Dhaka Med Coll. 2017; 26(2):148–52.
- Manzke H, Kruse K. Physiology and pathophysiology of calcium and phosphate metabolism in newborn infants. Personal study results and literature references. Monthly Prescription Paediatr. 1984;132(4):203–9. Available from: https://pubmed.ncbi.nlm.nih.gov/6328287/
- Mrelashvili, A., Russ, J.B., Ferriero, D.M. et al. The Sarnat score for neonatal encephalopathy: looking back and moving forward. Pediatr Res 88, 824–825 (2020). https://doi.org/10.1038/s41390-020-01143-5
- Jajoo D, Kumar A, Shankar R, Bhargava V. Effect of birth aspb hyxia on serum calcium levels in neonates. Indian J Pediatr. 1995;62(4):455–9. doi: 10.1007/BF02755067.
- Schedewie HK, Odell WD, Fisher DA, Krutzik SR, Dodge M, Cousins L, et al. Parathormone and perinatal calcium homeostasis. Pediatr Res. 1979;13(1):1–6. doi: 10.1203/00006450-197901000-00001.
- Mimouni F, Mimouni CP, Loughead JL, Tsang RC. A case-control study of hypocalcemia in high-risk neonates: racial, but no seasonal differences. J Am Coll Nutr. 1991;10(3):196–9. doi: 10.1080/07315724.1991.10718144.
- Saha D, Ali MA, Haque MA, Ahmed MS, Sutradhar PK, Latif T, et al. Association of hypoglycemia, hypocalcemia and hypomagnesemia in neonates with perinatal asphyxia. Mymensingh Med J MMJ. 2015;24(2):244–50.
- Getaneh FB, Adimasu M, Misganaw NM, Jember DA, Mihretie DB, Abeway S, et al. Survival and predictors of asphyxia among neonates admitted in neonatal intensive care units of public hospitals of Addis Ababa, Ethiopia, 2021: a retrospective follow-up study. BMC Pediatr. 2022;22(1):1–3. https://doi.org/10.1186/s12887-022-03238-w
- Samaiya PK, Krishnamurthy S, Kumar A. Mitochondrial dysfunction in perinatal asphyxia: role in pathogenesis and potential therapeutic interventions. Mol Cell Biochem. 2021;476:4421–34. https://doi.org/10.1007/s11010-021-04253-8
- Mota-Rojas D, Villanueva-García D, Solimano A, Muns R, Ibarra-Ríos D, Mota-Reyes A. Pathophysiology of perinatal asphyxia in humans and animal models. Biomedicines. 2022;10(2):347–51. https://doi.org/10.3390/biomedicines10020347
- Panwar AS, Taksande A, Kher A, Injeti G. Determination of serum electrolyte and calcium abnormalities in neonates with birth Asphyxia. J Pharm Res Int. 2021;23:807–15. https://doi.org/10.9734/jpri%2F2021%2Fv33i60B34683
- Behrman RE, Tsang RC, Chen I, Hayes W, Atkinson W, Atherton H, et al. Neonatal hypocalcemia in infants with birth asphyxia. J Pediatr. 1974;84(3):428–33. doi: 10.1016/s0022-3476(74)80733-x.
- Vuralli D. Clinical approach to hypocalcemia in newborn period and infancy: who should be treated? Int J Pediatr. 19;2019:1–7. https://doi.org/10.1155/2019/4318075