Biomedica - Official Journal of University of Health Sciences, Lahore, Pakistan
Volume 40(2):69-77
REVIEW ARTICLE
From chisels to lasers: a narrative of history of dentistry in the Indo-Pak Subcontinent
Afeera Rahat1
Received: 13 March 2024 Revised date: 21 May 2024 Accepted: 06 June 2024
Correspondence to: Afeera Rahat
*General Dentist, Rawalpindi, Pakistan.
Email: afeeraarahat@yahoo.com
Full list of author information is available at the end of the article.
ABSTRACT
This review highlights the rich heritage of dentistry in the Indian subcontinent and the diverse influences that have shaped its evolution. The roots of dentistry can be traced back to the inhabitants of the Indo-Pak subcontinent at Mehrgarh where the earliest evidence of dental practices was found. By analyzing the methods of the primitive “tooth-pullers” to those of modern-day specialists, this study delves deep into the influence of Ayurveda, Unani medicine, colonialism, and global exchanges on the field of dentistry.
This review comprises of the analysis of Ayurvedic records which document early dental procedures and the use of herbal remedies for oral diseases followed by the exploration of colonialism and the effect of Western medicine on shaping oral health practices. The dual system of healthcare prevailed due to the incorporation of traditional and modern medicine.
Furthermore, the key milestones are discussed. Alongside the developments, the study also discusses the challenges faced in achieving those developments and the initiatives launched that aimed at improving the quality of care provided. Patterns that led to the development of dentistry can be recognized which will help in further improvement.
In conclusion, the transition of dentistry from primitive practices to modern procedures is mainly due to the interaction between tradition and modernization. The findings of the paper underscore the need for improvement in research standards and a greater focus on public health by adopting both, traditional and modern-day medicine.
Keywords:
Dentistry, Pakistan, history, ayurvedic medicine, modernization.
Background
Dentistry as a profession has helped in shaping modern medicine. The history of dentistry is very rich, particularly in the subcontinent. It started with traditional healers and general physicians being primary dental healthcare providers. As the need grew, the field of dentistry started flourishing and started to make its mark upon the world. In this region, dentistry was especially influenced by traditional practices, religious beliefs, and societal norms. Infusion of Western medicine eradicated the false beliefs and myths associated with dental diseases such as caries being caused by worms and the association of rabbits with cleft lip. It improved the accuracy of the treatment, quality of care provided by the dentists as well as the comfort of patients.
The history of dentistry dates back to the first dentists in the world settled in Mehrgarh, Pakistan. They later became Indus Valley settlers. Unearthed ancient relics provide findings regarding the earliest dental practices. Later, ayurvedic medicine became the basis of healthcare. Similarly, during the medieval era, Unani medicine made its way from the Greeks to the subcontinent through Arabs. During the colonial time, modern practices made their way gradually replacing traditional oral health care. Today, despite considerable advancements and progressions, there remains ample room for further enhancing public health and dental knowledge throughout the region.
Fields such as tele-dentistry and forensic dentistry are being developed every day. With rapidly expanding technology, we are yet to see the marvels of dentistry. computer-aided design and computer-aided manufacturing (CAD/CAM), biomimetic restorative materials, and laser techniques can revolutionize dental care, enabling accurate and minimally invasive procedures, and ultimately leading to superior patient outcomes. These are the future scopes of dentistry in South Asia. Furthermore, improving the quality of research and analysis regarding the field will prove to be beneficial.
The research aims to explore the colorful history of dentistry in the subcontinent intertwined with different cultures by examining social, economic, and political factors that shaped the field. In this way, a comprehensive understanding of its evolution can be developed. The scope of the study is wide including topics such as traditional healing practices, holistic approach to dentistry, myths regarding dental ailments, and Western medicine. We see the evolution of the development of awareness among the general population with the advent of science and access to technology.
Methods
A systematic search was conducted across multiple databases including PubMed, Google Scholar, archives on the internet, and online journal websites. Keywords such as “dentistry history,” “oral health evolution,” and “subcontinent dental practices” were used to identify relevant articles, books, and scholarly literature. A blog1 was consulted containing related information followed by manual searches of reference lists. Additionally, manual searches were conducted from other identified sources to ensure comprehensive coverage of the topic.
The selection process involved screening titles and abstracts to include studies pertinent to the history of dentistry in the subcontinent. Articles were included if they provided insights into the evolution of dental practices, techniques, and societal perceptions across different periods.
Data extraction was performed systematically, focusing on major historical milestones, significant developments in dental techniques, and societal attitudes toward oral health. Finally, data synthesis involved organizing extracted information thematically to highlight major trends and shifts in dental practices over time.
Results
Primitive practices
Settlements in Baluchistan have provided the earliest known records of dentistry2. Bodies of prehistoric humans with dental work were discovered at Mehrgarh, Baluchistan. They had known the art of dentistry since the New Stone Age. Later during the Copper Age, they discovered the lost wax casting process.
Coppa et al report that 9 adult bodies were excavated. Further inspection revealed that they had their molars drilled as shown in Figure 13. Evidence suggested that drilling was done on live subjects using flint tips made with bones or stones4. Researchers were also sure that they used a type of filling but it did not survive.
There is also evidence of labret use5. Several tooth features such as worn facets of teeth, micro-chipping of some facets, and polishing of the labial/buccal surfaces suggest the use of labrets or plugs by the people. Another argument suggests carrying pebbles by mouth resulting in these features. More work needs to be done to document and describe these non-occlusal facets.
Ayurveda
Ayurveda is known to be a complete medical system that has made important contributions to many sectors, including dentistry. Charaka Samhita and Sushruta Samhita are among its oldest surviving texts dating back from 1,500 before common era6.
Charaka Samhita focuses on general medicine while Sushruta Samhita on general surgery. The Latter contains 186 chapters7 and is divided into 2 parts and 6 books. Several ailments of the oral cavity are described along with surgical instruments, techniques, and herbal treatments. It also contains material describing ways in which practitioners can guide their disciples like teaching the art of extraction on jackfruit and dead animals. Additionally, cauterization techniques are to be demonstrated on sensitive tissue areas.
There is evidence for the use of prosthetic teeth in medieval India. In 1194 CE, King Jai Chandra sustained serious injuries in a war. He was later recognized by his set of artificial teeth which were affixed by gold wires8.
Till 15th Century
With each passing year, advancements started happening in all fields, including dentistry. Dental care practices in this area were influenced by cultural beliefs, societal norms, and local traditions. Methods employed for maintaining oral hygiene were the use of chewing sticks and use of herbal tooth powders and mouth rinses. Healthcare was administered by traditional healers, called Vaidyas, who practiced Ayurveda or other indigenous medical systems. Owing to the absence of sophisticated technology, dental care primarily relied upon natural remedies and rudimentary procedures9. Ladies of royal household would have gold, jade, and diamond inlays in their teeth. Gold restorations on the labial sides of incisors were also common for caste distinction10.
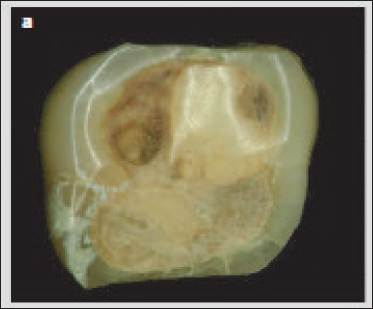
Figure 1. Drilled molar excavated at Mehrgarh.
16th and 17th Century
This era was marked by the infiltration of Western knowledge into traditional practices due to the increased influence of Europeans. Dentistry practices previously deeply influenced by religious, cultural, and societal beliefs, gradually started to adopt a modern look.
Although introduced in the 12th century during the Delhi sultanate by the Arabs, it was in the 16th century that Unani medicine started flourishing in the South Asian region under Mughal rule. The practitioners of this medicine were called Hakims and are still found today in various regions. The system also started incorporating the methods of Ayurveda11.
18th Century
During the 18th century, the establishment of the British East India Company expanded the Western influence in the region. European settlers and officials often brought their own medical practitioners which resulted in the introduction of new dental instruments and modern techniques. Small dispensaries and hospitals were set up by the British only to serve the European employees or the military. The caste system and societal hierarchies influenced the accessibility and type of dental care available to different population segments12.
The exchange of medical knowledge between the British and the local practitioners in India was mutual, with both sides benefiting from each other’s expertise12. In the late 18th century, British medical professionals developed a keen interest in Indian surgical techniques, particularly those related to skin grafting for facial reconstruction. These traditional Indian practices laid the groundwork for the development of contemporary plastic surgery8.
19th Century
The medical records from the 19th century are often seen to racialize the dental differences in different practices. Caries were commonly associated with the “civilized white races,” whereas the tooth loss observed among local populations was attributed to gingival infection due to excessive calculus deposits, and habitual consumption of betel leaf and areca nut. Additionally, South Asian dentition was often characterized as “uniformly large, strong, and exceptionally well developed with the third molars and lateral incisors developed proportionally with the other teeth”13.
Periodontitis was widespread, especially in the Europeans and high-class natives but not in the poor class owing to their coarse diets. The practice was more inclined toward replacement rather than rehabilitation because of the low cost of artificial teeth14. Figure 2 shows primitive dental prosthesis as practiced by Indian dentists consisting of artificial ivory tooth affixed to natural teeth using gold wires and thread ligatures15.
There existed a professional rivalry between physicians and dentists. Dentists were not well-received socially as well as professionally unless enrolled in military service14.
Formal dental education was not widespread in the early 19th century. Some individuals pursued education and training in dentistry through apprenticeships with European dentists or by studying abroad. In 1848, the first dental college was established in Baltimore, USA, offering a Doctor of Dental Surgery (DDS) degree. This was a pivotal moment for the field of dentistry worldwide because, for the first time, dentistry was seen as a distinct profession requiring specialized training resulting in the professionalization of the field. In the subcontinent dental schools and colleges were established in major cities such as Calcutta (now Kolkata), Bombay (now Mumbai), and Madras (now Chennai) by the latter half of the century. These institutions provided training in Western dental science and techniques.
In the rural areas, however, modern practices and resources were unavailable. Hence traditional practitioners, i.e., Vaidyas or Hakims were still taking up the role of dental healthcare providers in their respective areas. It was believed that worms were responsible for causing dental caries. Women from the gypsy tribe were known to take out these worms16.
The Indo-Pak subcontinent saw advancements in anesthesia, pain management, and dental materials around this time. This contributed to improvements in dental care during this period16,17.
In the 19th century, India and China were appraised for their numerous contributions to the field of medicine15. They are also believed to be the inventors of toothbrushes as they used to chew twigs giving their breath a pleasant odor. This led to the invention of the toothbrush18.
European medical professionals continued to take a keen interest in traditional practices. They wrote various texts documenting their observations. One such text by Watt19 delineates the use of borax, plants, and gold leaf in dentistry for the treatment of oral ailments as well as for making prosthetic teeth.
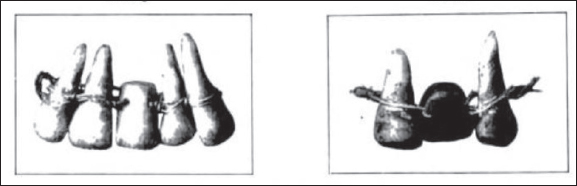
Figure 2. Ancient dental prosthesis comprising of ivory and natural human teeth fixed with a gold wire (A) and thread ligature (B).
Under the influence of Westernization and with the introduction of anesthesia, surgical procedures were performed using contemporary techniques. One such case is mentioned in Transactions of the Medical and Physical Society of Bombay20 in which a tumor was successfully removed from a woman’s mouth by a group of surgeons at Camp Deesa, Gujrat, India. As the traditional medical practices were still ongoing, it is mentioned in the text that previously by the advice of some of her friends, a horse hair ligature was applied around the tumor. Due to this, a small portion of its extremity was removed. It grew again and the method was repeated. But every time the tumor regained its original size.
In the 1860 edition, a case is detailed of a patient who presented with nevus above the upper lip extending to the mucous membrane of the upper lip and cheek. Treatment attempts were undertaken which included strangulation of swelling above the upper lip with strong double silk thread passed through needles at the base of the tumor. The ligatures were cut and the tumor was strongly tied in four places. By the fifth day, the strangulated portion had sloughed off leaving behind an ulcer, which healed in a fortnight. It was later decided to leave the major, more formidable part of the swelling alone due to the risk of hemorrhage and sloughing off inside the mouth21.
In multiple publications, herbal treatment for scurvy is discussed22,23.
In an alternative account, it was discussed that goldsmiths practiced dentistry due to acquired knowledge. They knocked out the mobile and painful teeth by gentle hammering, bound the teeth with gold and silver wires, and also fixed artificial teeth made of ivory, conch, or bone in the mouths of the patients. It was also observed that over time goldsmiths adopted Western practices and started using proper forceps for extractions, prescribed medicines for toothaches, and mastered the art of making artificial teeth by spring as did the Europeans24.
Various newspapers like The Madras Mail and Amrita Bazar Patrika have published advertisements regarding artificial teeth marketing their products as “cheap,”25 “manufactured in the latest American style and principle,” and “durable, good-looking, and as strong as the natural ones”26.
Women also stood with men in this field. There was an advertisement as shown in Figure 3, published in Amrita Bazar Patrika, 1989 of a female dentist who was the daughter of another dentist. She sold artificial teeth and advertised herself as a dentist for women who observe purdah27.
20th Century
This was the era of professionalization and standardization of dental practices throughout the region. Extensive work was done in the field of research.
In the historical records of dentistry, racial slurs are substantially observed. In Dr. Henry Lovejoy’s book, Indian dentists are portrayed in a derogatory light as being “natives, bad and indifferent”28. The observation was set before the publishing of the Indian Act for Dentists. Hence, dentistry was open for anyone to practice.
On top of that, there was an absence of dental journals and societies in the region and the dominance of dental literature in the English language rather than the native languages. These complicating matters posed a serious challenge in the name of forming a cohesive dental community.
Description of some dental clinics from the region at the time included dentists and patients sitting on the floor due to the absence of chairs or stools. Clinics of a very few dentists particularly the English ones used dental chairs, engines, and proper instruments.
The prevalence of unqualified practitioners further compounded the problem. They would practice under the apprenticeship of English dentists and then open their practices from the experience they had gained, offering the services at lower rates than the qualified ones. Despite this, technological advances continued to make their mark. Amalgam and cement fillings were widely used in the region as well as vulcanite dentures. Oral hygiene methods ranged from traditional practices such as using Nim tree branches as toothbrushes, using mud to clean teeth, rinsing the mouth, and cleaning teeth while bathing in the ponds or wells to using modern international brands’ dentifrices, including Colgate, Sozodont, Floriline, and Graves28.
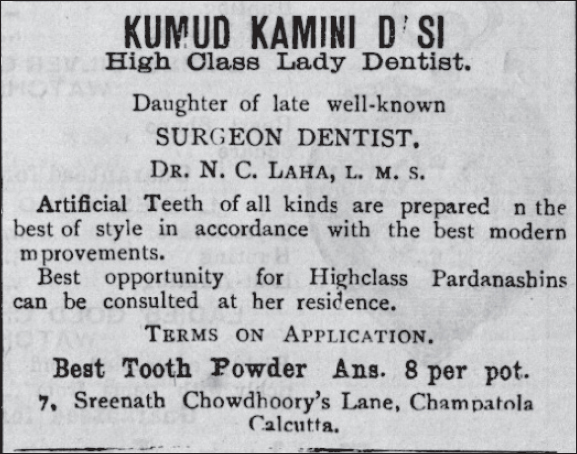
Figure 3. Advertisement published in Amrita Bazar Patrika, 1989 about a female dentist offering services for artificial teeth.
Dr. Khambatta in another account paints a horrific picture of dental practices going on at the time29. With a population of 350,000,000, there were only 5,000 dentists in India, 95% of whom were quacks. Although there were several government-owned medical colleges, there was only one dental institution, that too privately owned. The government paid no attention to the importance of dental education, or dental health on the whole. Chewing of betelnut and pan chewing was fairly common resulting in bad oral health in the general population. Another reason for negligence to oral health was the purdah system, where women wanted to be treated by female dentists only but there were only 6 female dentists in the whole of India. There was a general scarcity of dental clinics and hospitals. 80% of the population suffered from oral diseases29.
Dozens of unqualified dental care providers were seen squatting by the roadside with extracted teeth, bottles of potions, dried herbs, and a jar of wriggling worms, allegedly removed from dental caries. Extraction of a tooth was seen as being synonymous with butchery or murder. Yet the qualified ones from the region were called on in neighboring countries to cater to the dental needs of affluent individuals. One such example is Mr. O Meara, the only dentist in Punjab at that time. He was called to Afghanistan by the Amir (King) for himself. This expedition lasted 6 months, and on his return, he recounted how the Amir had him perform extractions on his courtiers before he himself was operated on30.
Belief in myths prevailed. Cleft lip or hare-lip, as they called it, was said to be associated with eating rabbit meat. It was believed that hare-lip occurs because of the charming of the mother by a rabbit imparting self-features to the baby31.
Dental education
By the end of the 19th century, the establishment of dental schools and institutions had already begun in the Indo-Pak subcontinent. This time around, they continued to evolve and expand their programs to meet the growing demand for dental professionals. Dr. Rafiuddin Ahmed (figure 3) was a dentist and educator (later a minister in the West Bengal cabinet) who obtained his DDS surgery from the University of Iowa, USA in 1919. Upon returning to his homeland, Dr. Ahmed played a pivotal role in advancing dental education by founding the Dr. R Ahmed Dental College and Hospital in Sealdah, Kolkata, in 1920 (Figure 4)32,33.
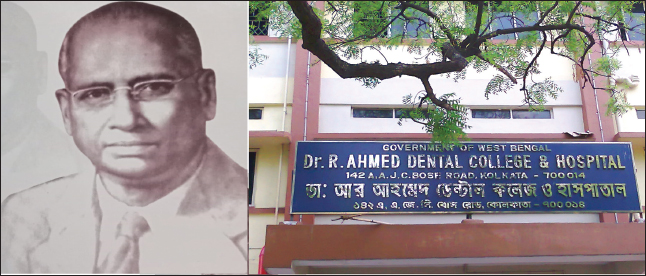
Figure 4. Dr. Rafiuddin Ahmed (left), Dr. R Ahmed Dental College and Hospital (right).
This was followed by the establishment of De’Montmorency College of Dentistry in Lahore in 1934. These institutions played a crucial role in laying a foundation for the development of the modern dental profession in the region. However, after the partition of India and Pakistan in 1947, already scarce resources were distributed. There were three dental colleges left in India and only one in Pakistan. In addition, the gradual advancement of dentistry in the region was disrupted by the migration of dentists as they shifted their loyalties based on religion30.34.
The Dental Act, 1948
In the early 1900s, there was no dental act or association. Small organizations existed that aimed at evolving dentistry. In the year 1946, the first All-India Dental Conference was held. It was decided to amalgamate all the small organizations into an All-India Dental Association adopting a uniform constitution that safeguarded both the qualified and the unqualified dentists who were practicing based on apprenticeship. In 1948, the Dental Act bill was passed. Only registered dentists were allowed to practice. Suddenly, there was a sharp depletion of the workforce and a loss of livelihood across the region. Hence, Part B was introduced which allowed the enrollment of unqualified dentists working for more than 5 years before the Act. In the year 1949, the Dental Council of India was formed with the sole purpose of regulating dental education and the profession. By the year 1955, India had a Dental Association, a Dental Act, two dental journals, and six dental colleges35.
Post-partition Pakistan
In Pakistan, there was only one dental college. Dental sections were later established at Liaquat Medical College (Hyderabad) in 1951, Khyber Medical College (Peshawar) in 1964, and Nishtar Medical College (Multan) in 1974. The dental practice could not rise to its full potential because it was continuously overshadowed by the medical profession and also due to unprofessional and ineffective leadership. In the United States of America, it was through dental journals that dentistry changed from a mechanical trade to a profession34. There was no journal at the time in Pakistan. Journal of the Pakistan Medical Association (1953) was the first journal to be published. Here too dentistry was under the shadow of medical sciences. Then, finally, in 1981, Pakistan Oral and Dental Journal was established as being the first journal specific to the field of dentistry36.
In the later part of the century, keeping in mind the need for specialists, College of Physicians and Surgeons, Pakistan, started the diploma of Membership of the Faculty of Dentistry which was later renamed the diploma of the Membership of the College of Physicians and Surgeons, Pakistan (MCPS, Pak). In 1994, major degree fellowships program in clinical disciplines of dentistry were started37.
Technology
Technological advancements such as radiographs, anesthesia techniques, and knowledge of previously unknown dental materials increased patient comfort and satisfaction. It also increased the ease and efficiency of the operator and the accuracy of the treatment.
Dental care for all
Standard dental care was no longer limited to the urban areas only. With the establishment of hospitals, clinics, and private practices in underprivileged areas, healthcare proliferated in rural areas providing preventive, restorative, and surgical care to the patients. With the improved access to healthcare, the oral health outcomes of the population improved.
In the 20th century, public health dentistry initiatives gained momentum. Indian Dental Association (IDA) was established in 1946. By acting as a regulatory body, it ensured that dental professionals across the country met established standards of care and practice38.
Multiple community dental programs such as free dental camps were arranged to provide essential dental care, especially in the underserved areas where access was difficult. Widespread campaigns were held through various mediums such as posters, pamphlets, radio broadcasts, and community events to raise awareness about oral health care. Fluoridation of water was adopted by several communities in the region to ensure optimal levels of fluoride in the drinking water.
One such example of this program was the initiatives undertaken in Pakistan by various organizations. Dental professionals visited schools to conduct oral health screening camps and provide preventive treatments such as dental sealants, fluoride applications, and oral health education sessions39.
In India, a similar program was the National Oral Health Program launched by the Government of India in 1986, which aimed to promote oral health education and preventive measures in schools40.
21st Century
Dentistry in the current century has seen magnificent changes throughout Pakistan and India. Modernization of techniques and technological advancements such as CAD/CAM, digital imaging, and laser dentistry have revolutionized dental treatments, making them more precise, less invasive, and often more comfortable for patients. There is an increased awareness about oral hygiene maintenance and regular dental checkups in the general population.
There has been a growing trend toward specialization within dentistry, with more dentists pursuing postgraduate education in related fields. This has enabled dentists to provide more specialized and comprehensive care to patients with specific dental needs.
However, challenges such as access to dental care in rural areas and affordability for low-income groups remain areas of concern that need to be addressed for further improvement in dental healthcare delivery.
There has been a massive surge in the population of Pakistan and India. With growing demand, resources begin to deplete slowly not being able to keep up with the ever-increasing demand. Despite great achievements in oral health, dental caries, and periodontal diseases remain a major global problem41.
Dental education
Dental education in India has undergone a revolutionary transformation to bring it into the 21st century. There are nearly 301 dental schools with a dentist-to-population ratio of 1:9,992 compared to 1:301,000 in the 1960s. However, due to poor systematic planning regarding the development of dental colleges and the affinity of graduating dentists to establish practice in developed centers, there is an uneven geographical distribution. Hence, oral health remains a commodity unknown to the majority41-43.
In Pakistan, almost all of the public and private medical colleges have established their dental departments. Currently, there are 61 dental colleges. However, many of these establishments lack the qualified teaching staff needed to ensure quality teaching and training for students. The institutions are not designed with factors such as the skills needs of the population, the demands of the job market, and oral health objectives in mind34.
There are 84 Pakistan Medical and Dental Council (PM&DC)-recognized journals out of which 4 are dental-specific44.
Public health
In the early 21st century, dental practice focused majorly on restorative approaches rather than preventive measures45. Gradually, the paradigm is shifting toward the conservative and preventive approach, prioritizing early intervention and enabling the general public to adopt healthier oral hygiene practices. Thereby, decreasing the overall disease load on the population46.
Digital dentistry and Tele-dentistry
The integration of digital technologies into the dental industry has brought about innovation and improved access to dental services, enhancing overall efficiency. Tele-dentistry is an amalgamation of information technology in dentistry and has the potential to offer promising prospects for advancing the field to new heights47.
Future Prospects
Diving into the future, it is apparent that a sea of endless possibilities lies ahead. There have been breakthrough innovations such as tele-dentistry, biomimetic restorative materials, tissue engineering, CAD/CAM, and AI-driven diagnostics. To keep up with the advancements already taking place in the world, existing resources should be channeled to make dental education and the dental workforce fit for future purposes. Dental care should be integrated into primary care to expand access to recommended treatments and promote better health overall. Pakistan Dental Council should be established to promote and safeguard the interest of dentistry as a discipline. Dental curricula should be revised to be brought on par with international standards.
Conclusion
During the literature review process, it was evident that substantial material regarding advancement in dentistry originated from India and very less from Pakistan. This highlights a pressing necessity to improve the standards of research and the overall dental infrastructure in Pakistan. Encouraging research initiatives and promoting evidence-based practice can elevate the standard of dental care.
Both countries have made significant strides in the field of dental education and research. Yet there remains ample room for improvement and growth. Public health initiatives, community programs, and school-based oral health education should be encouraged as a part of preventive dentistry. Forensic dentistry is an emerging field across the world. There exists a need to give more attention to incorporating it into the curriculum.
In addition, more research needs to be done on integrating traditional ways with modern dental practices. In this way, we can respect and preserve the rich cultural heritage, providing a holistic approach to oral health in the region. It can also prove to be cost-effective.
Limitations of the review article
The study was limited by the availability and accessibility of historical records and archaeological findings. Due to the historical nature of the research, there may be gaps or inconsistencies in the data. The scope of the study was limited to the subcontinent, and findings may not be generalizable to other regions.
List of Abbreviations
| BCE | Before Common Era |
| CAD/CAM | Computer-Aided Design/Computer-Aided Manufacturing |
Conflict of interest
None to declare.
Grant support or financial disclosure
None to disclose.
Ethical approval
Not applicable.
Author’s contributions
AR: Conception and design of study, acquisition of the data, drafting of manuscript, critical intellectual input, and approval of the final version of the manuscript to be published.
Authors’ Details
Afeera Rahat1
- General Dentist, Rawalpindi, Pakistan
References
- Nair A. Of heavenly twins, gold wires and wooden teeth: dentures and dentistry in colonial and precolonial India [Internet]. Lives worth living: disability histories. 2018. Available from: https://disabilitystories.com/2018/01/06/of-heavenly-twins-gold-wires-and-wooden-teeth-dentures-and-dentistry-in-colonial-and-precolonial-india/#_ftn11
- Jarrige JF, Jarrige C, Quivron G, Wengler L, Sarmiento Castillo D. Mehrgarh. Neolithic period - seasons 1997-2000: Pakistan. 1st ed. Vol. 15. Paris, France: Editions de Boccard; 2013.
- Coppa A, Bondioli L, Cucina A, Frayer D, Jarrige C, Jarrige J, et al. Palaeontology: early neolithic tradition of dentistry [Photograph]. Nature. 2006;440(7085):755–6. https://doi.org/10.1038/440755a
- Coppa A, Bondioli L, Cucina A, Frayer DW, Jarrige C, Jarrige JF, et al. Early neolithic tradition of dentistry. Nature. 2006;440(7085): 755–6. https://doi.org/10.1038/440755a
- Frayer D, Nava A, Tartaglia G, Vidale M, Coppa A, Bondioli L. Evidence for labret use in prehistory. Bull Int Assoc Paleodont. 2020;14(1):1–23.
- Schultheisz E. History of physiology. Oxford: Oxford, UK: Pergamon Press; 1981. 60–1 pp.
- An English translation of the Sushruta samhita, based on original Sanskrit text. Edited and published by Kaviraj Kunja Lal Bhishagratna. With a full and comprehensive introd., translation of different readings, notes, comperative views, index, glossary and plates. Susruta, Bhishagratna, Lal K, Kaviraj. Calcutta, India: Wilkins Press; 1999.
- Selin H, editor. Encyclopaedia of the history of science, technology, and medicine in non-western cultures. Berlin, Germany: Springer; 2008. https://doi.org/10.1007/978-94-017-1416-7.
- Sharma PV, Indian National Science Academy. History of medicine in India, from antiquity to 1000 A.D. New Delhi, India: Indian National Science Academy; 1992.
- Choksey KM. Dentistry in ancient India. News Bull Indian Dent Assoc. 1974;5(1,2):9–12.
- Schmidt Stiedenroth K. Unani medicine in the making: practices and representations in 21st-century India. Amsterdam, The Netherlands: Amsterdam University Press; 2020. https://doi.org/10.2307/j.ctv131bsw5
- Saini A. Physicians of colonial India (1757-1900). J Family Med Prim Care. 2016;5(3):528–32. https://doi.org/10.4103/2249-4863.197257
- Egbert JW. Teeth of Indian nations. In: Kirk EC, editor. The dental cosmos: a monthly record of dental science. Philadelphia, PA: White dental manufacturing company; 1900. 42(1-6):61.
- Lundy EA. Dentistry in India. In: Pacific stomatological gazette. JW Edwards The Ohio State, USA. 1896;4:302–8. Available from: https://books.google.com.pk/books?id=Pbo1AQAAMAAJ
- Guerini V. A history of dentistry from the most ancient times until the end of the eighteenth century. Lea & Philadelphia and New York. 1909. p 30.
- Crooke W. The popular religion and folk-lore of northern India. A. Chapter 3, The godlings of disease. Constable & Company; 1896. p 151. Available from: https://books.google.com.pk/books?id=CjDXAAAAMAAJ
- Ilic DV, Radicevic BA, Nedelcheva A, Djurovic I, Ostojic D. Traditional dentistry knowledge among serbs in several Balkan countries. J Intercult Ethnopharmacol. 2017;6(2):223–33. https://doi.org/10.5455/jice.20170325055450
- Kapoor PC, editor. Civic affairs. Citizen Press CA. Vol. 4, 1957.
- Watt G. A dictionary of the economic products of India. Vol. 1, 1889. Calcutta India. Available from: https://books.google.com.pk/books?id=89ku-rP4aS8C&printsec=frontcover&source=gbs_ge_summary_r&cad=0#v=onepage&q&f=false
- Cameron WL. Removal of a large tumor from the mouth. Trans Med Phys Soc Bombay. 1849;9:217–9.
- Rustomjee B. Nevus of the parts above the left upper lip and interior of the mouth causing deformity of the face. Trans Med Phys Soc Bombay. 1860;6(New Series).
- Transactions of the Medical and Physical Society of Bombay. Bombay, India: American Mission Press; Volume 3, 1840. ,
- Macdowall C. Further remarks on new theories of and new cures for scurvy. Trans Med Phys Soc Bombay. 1884;4(New series):22–3. Available from: https://books.google.com.pk/books/about/Transactions_of_the_Medical_and_Physical.html?id=nZ8EAAAAQAAJ
- Arjun S. The practice of medicine in Bombay. Trans Med Phys Soc Bombay. 1883;3(New series):1–24. Available from: https://books.google.com.pk/books/about/Transactions.html?id=TSegAAAAMAAJ
- Amrita Bazar Patrika. Newspaper Advertisement. 1897;Aug 14;30(190).
- Amrita Bazar Patrika. Newspaper Advertisement. 1900 Nov 13;32(252).
- Dasi KK. Amrita Bazar Patrika. Newspaper 1899 Jan 26;30(18):2.
- Ambler HL. Around the World Dentistry. Cleveland, OH: Judson Printing Co; 1910.
- Khambatta SM. The present status of dentistry in India. J Am Dent Assoc. 1928;15(2):252–5. https://doi.org/10.14219/jada.archive.1928.0047
- Kochhar PC, editor. History of the army dental corps and military dentistry. New Delhi, India: Lancer Publishers & Distributors; 2000.
- Eastman CA, Blumenschein EL. Indian boyhood. Dovers Publications, NY, USA. Available online at: https://www.amazon.com/Indian-Boyhood-American-Charles-Eastman/dp/0486220370; 1971.
- University Dental College. A short history of modern dentistry practices in Bangladesh [Internet]. Dhaka: University Dental College; [cited 2024 Feb 21]. Available from: https://www.udchbd.com/a-short-history-of-modern-dentistry-practices-in-bangladesh/
- Wikimedia Commons. [cited 2024 May 25]. Available from https://commons.wikimedia.org/
- Jawaid SA. Plight of dentistry in Pakistan. Pak J Med Sci. 2020;36(3):299–302. https://doi.org/10.12669/pjms.36.3.2278
- Mehta FS. Dental progress in India. J Am Dent Assoc. 1955;50(5):527–31. https://doi.org/10.14219/jada.archive.1955.0093
- Pakistan oral and dental journal. About PODJ [Internet]. Karachi: PODJ;[ [cited 2024 May 21].]. Available from: https://podj.com.pk/index.php/podj/about-podj
- Ghani F. Prosthodontics as a dental specialty in Pakistan: reflections on its historical developments, achievements, and future plans. J Pak Prosthodont Assoc. 2013;1(2):65–72.
- Indian Dental Association. About IDA [Internet]. Mumbai, India: Indian Dental Association; [cited 2024 May 22].]. Available from: https://www.ida.org.in/AboutUs/Details/About-IDA
- Haleem A, Khan AA. School-based dental health education in Pakistan -the need and possible strategies. Pak Oral Dent J. 2006;26(1):119–24.
- National Oral Health Programme. About us [Internet]. [cited 2024 May 22].Available from: https://edantseva.gov.in/content/national-oral-health-programme
- Parkash H, Duggal R, Mathur V. Guidelines for meaningful and effective utilization of available manpower at dental colleges for primary prevention of oro-dental problems in the country. GOI-WHO Collab Project. 2007(1):1-56. Availble online at: https://screening.iarc.fr/doc/Oral_Health_Oro-Dental_Problem_WHO_Project_Guidelines.pdf.
- Hayashi M, Haapasalo M, Imazato S, Lee JI, Momoi Y, Murakami S, et al. Dentistry in the 21st century: challenges of a globalizing world. Int Dent J. 2014 Dec;64(6):333–42. https://doi.org/10.1111/idj.12132
- Jaiswal AK, Srinivas P, Suresh S. Dental manpower in India: changing trends since 1920. Int Dent J. 2014;64(4):213–8. https://doi.org/10.1111/idj.12111
- Pakistan Medical & Dental Council. (2024). List of PM&DC Recognized Journals. Available from https://pmdc.pk/Documents/Letters/recognized-updated-journals-2024.pdf
- Niaz MO, Naseem M, Siddiqui SN, Khurshid Z. An outline of the oral health challenges in “Pakistani” population and a discussion of approaches to these challenges. J Pak Dent Assoc. 2013;22(3):215–23.
- Bukhari SGA, Usman CM, Ehsan A, Aziz N. Analysis of referral patterns and health care work force (dental surgeons) in AFID. Pak Armed Forces Med J. 2021;67(SUPPL-1):S104–07.
- Khan SA, Khalid N, Bajwa O, Tariq A, Naqvi Z. Tele-dentistry during Covid-19 pandemic; perceptions of dentists in Pakistan. Pakistan J Med Health Sci. 2022;16(9):417. https://doi.org/10.53350/pjmhs22169417
Keywords: Dentistry, Pakistan, History, Ayurvedic Medicine, Modernization.

Publication History
Received: March 13, 2024
Revised: May 21, 2024
Accepted: June 06, 2024
Published: June 25, 2024
Authors
Afeera Rahat
General Dentist, Rawalpindi, Pakistan