Biomedica - Official Journal of University of Health Sciences, Lahore, Pakistan
Volume 37(2):123-129
ORIGINAL ARTICLE
The evaluation, management, and outcome about an experience with sharp force abdominal injury
Zhou Xu1, Yunsong Lu1, Heng Li1, Dailiang Peng1, Xuwei Jiang1, Yubin Kou1*
Received: 26 March 2021 Revised date: 17 May 2021 Accepted: 04 June 2021
Correspondence to: Yubin Kou
*General Surgery Department, Shanghai Baoshan District Hospital of Integrated Traditional and Western Medicine, Shanghai, China.
Email: koagrace@sina.com
Full list of author information is available at the end of the article.
ABSTRACT
Background and Objective:
Sharp force injuries (SFI), which are inflicted by cutting or stabbing, result in variable outcomes depending upon the nature and site of injury. This study evaluated the cases of SFIs and their outcome with reference to the time of presentation, demographic data, wounded organs, and surgical procedures performed.
Methods:
This retrospective study analyzed the clinical data of 20 patients who presented with sharp force injury (knife stabbing and penetrating abdominal trauma) and were admitted between April 2015 and November 2016. The management and outcome of patients were recorded.
Results:
All patients in this study were male and aged between 21 and 30 years. Knife stabbing was the only mechanism of injury in all cases. Colon (50%) was the commonest organ injured followed by intestine (40%) and liver (30%). Mortality rate was 10%. There were two cases with negative laparotomy (10%). Wound sepsis (10%) was the commonest complication.
Conclusions:
SFI involving abdominal area are managed either conservatively or with primary repair and laparotomy to save internal organs. Early presentation and prompt management leads to reduced chances of complications and mortality.
Keywords:
Sharp force injury, Retrospective, Abdominal injury, Evaluation, Outcome, Complication.
Introduction
Sharp force injury (SFI) is an injury inflicted by cutting or stabbing [1]. In recent years, due to the significant increase in the incidence of emergency trauma, SFI has become the focus of public attention [2,3]. It is noteworthy that about 10% of all trauma-related deaths occur due to blunt or penetrating abdominal injuries [4]. The abdomen is one of the most common parts of SFI. Abdominal SFI is an emergency, and without properly treated in time, it will cause serious consequences [5]. Although the identification, diagnosis and management of abdominal SFI have improved in recent years, there is still a high mortality rate. At present, the best treatment for patients with abdominal SFI has not yet been fully elucidated [6] Most patients with abdominal SFI need immediate laparotomy, especially those with shock, extensive peritonitis, and evisceration [7,8]. It is still controversial for patients with asymptomatic or signs of peritonitis, because the mandatory laparotomy in this group of patients may lead to unacceptable negative laparotomy [9]. For patients without peritoneal penetration, peritoneal penetration with no visceral injury or peritoneal penetration with insignificant visceral injury, there may be no obvious symptoms or mild symptoms [10]. This group of patients had to undergo ongoing clinical evaluation, local wound exploration, computed tomography (CT), and diagnostic laparoscopy to determine whether they needed delayed laparotomy.
However, there are few studies on the patterns of wound and organ damage in SFI cases. Therefore, in the current study, we aimed to investigate the epidemiological characteristics, patterns of injury, morbidity, mortality, and disposal of abdominal SFI in a clinical setting.
Methods
A total of 20 patients with sharp force injury (knife stabbing and penetrating abdominal trauma) were admitted to the Department of General Surgery, Shanghai Baoshan District Hospital, Shanghai, China l from April 2015 to November 2016. The diagnosis of sharp force injury was made according to the initial resuscitation, detailed clinical history, laboratory tests, CT scan, X-ray ultrasonography, and physical examination. All patients were studied for various variables, including age, gender, time of presentation, signs and symptoms, various procedures employed, postoperative complications, and mortality.
Statistical analysis
Data were analyzed using the Statistical Package for the Social Sciences software (version 22.0). Quantitative data were shown as mean ± standard deviation while qualitative variables were presented as frequency or percentages.
Results
This study included 20 patients (all males) with a mean age of 23.7 ± 2.1 years (Figure 1). All patients suffered penetrating trauma to the abdomen by knife. There were n = 12 cases (60%) with only one wound and n = 8 cases (40%) with two or more wounds.
Twelve patients (60%) experienced abdominal pain and presented bleeding; six patients (30%) had hypovolemic shock; and one patient (10%) presented with hematuria. Physical signs included generalized abdominal tenderness and guarding in (100%) patients. One case died within minutes of presentation because of blood loss more than 4,000 ml in spite of aggressive and prompt fluid resuscitation.
Ten patients (50%) presented within 2 hours of the injury while 8 patients (40%) within 4 hours and 2 (10%) presented more than 6 hours after injury.
There were 10 cases (50%) with colon injury, 8 cases (40%) with intestine trauma, and 6 cases (30%) with liver damage (Figure 2). Commonest surgery was colostomy that was performed in 10 (50%) patients. Primary bowel repair was performed in 8 (60%) patients, liver injury closure and mesenteric repair were performed in 6 (50%) and 4 (15%) patients, respectively. Only one patient (5%) had splenectomy.
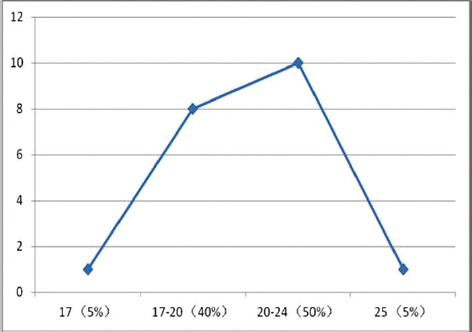
Figure 1. Age distribution of patients (year).
Mortality rate was 5%; in one case only because of fatal blood loss followed by cardiopulmonary arrest. Most frequently observed post-operative complication was wound infection in four cases (20%) followed by wound dehiscence and abscess in 1 case (5%) each. Rest of the patients recovered without any adverse events.
Discussion
Penetrating abdominal injuries are a frequent emergency and may cause considerable troubles at emergency service [11]. Karamercan et al. [12] concluded that approximately 10% of all trauma-related deaths occurred as a result of blunt or penetrating abdominal injuries. Patients who have persistent hypovolemic shock due to continuous blood loss in spite of aggressive fluid resuscitation require an urgent laparotomy [9]. Non-operative management maybe is an alternative approach for hemodynamically stable solid organ injuries to avoid negative laparotomy. Focused assessment with sonography for trauma (FAST) is a helpful diagnostic tool which is frequently used in the non-therapeutic surgical procedures [13]. Sonography is widely used as it is inexpensive, portable, non-invasive, highly sensitive, repeatable, and not involving X-ray, easily applied by clinicians and enabled a rapid response in about 4-5 minutes [3,6]. FAST and CT help guide treatment for stable with penetrating sharp injuries to the abdomen and are beneficial to detect patients with minimal and clinically undetectable signs of abdominal injury and have become part of current management guidelines [7-9,14].
In our study, the patients with free fluid or with suspected solid organs injury, CT was used to perform further investigation and to evaluate the injury and this also was recommended in one article [15]. The colon and intestine were the most commonly injured hollow organ, liver is the most commonly injured solid organ as a result of knife stabbing injury in our study. Blood loss is fatal for patients with penetrating liver injury. Gastric juice, intestinal juice, and gastrointestinal contents of the hollow organs may cause peritoneal irritation. There is necessity of emergency laparotomy in patients with signs of peritoneal irritation because of digestive tract rupture or hemodynamic instability following penetrating injury [16,17]. There were two cases with negative laparotomy in our study. The intestine and greater omentum of two patients were exposed because of knife stab injury and were performed operation.
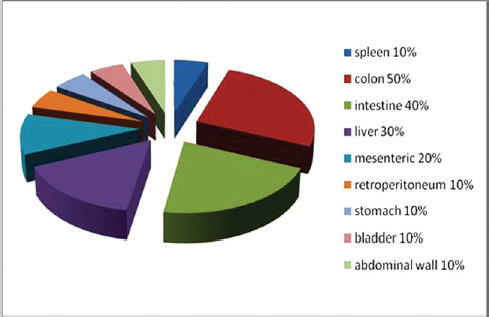
Figure 2. Distribution of organ injuries.
Time of presentation is very important for life-saving and patients presented within a short time can reduce the mortality [18]. In this study, the less time the patients arrived at hospital after injury with the better outcome of treatment and less complications after operations. Mortality rate was seen in n = 1 (5%) case because of fatal blood loss followed by cardiopulmonary arrest. The major cause of death was delayed presentation to hospital with continuous blood loss. Early presentation of patients helps surgeon to start appropriate resuscitation on time. These infections were managed conservatively and one case (colon penetrating injury) treated by continuous abdominal double cannula lavage and low negative pressure drainage.
Conclusion
In this study, we evaluated the diagnosis and management of 20 cases with SFIs, including time of presentation of patients, demographic data, wounded organs, surgical procedure, and outcomes. These results suggest that correct diagnosis, early resuscitation, and prompt evaluation, which form the most vital part of SFI management, may prevent death of patients.
Limitation of the study
The limitations of the current study include: a relatively small sample size; and a single-center and retrospective design.
Acknowledgement
The authors would like to acknowledge the staff of Surgical Department of Shanghai Baoshan District Hospital of Integrated Traditional and Western Medicine, Shanghai, China for their support during data collection
Conflict of interest
None to declare.
Grand support & financial disclosure
None to disclose.
Ethical approval
The ethic approval was obtained from the Ethic Committee of Shanghai Baoshan District Hospital of Integrated Traditional and Western Medicine, Shanghai, China. (Approval No. 2015024)
Authors’ contributions
ZX, HL, and YSL: Conception and design of study, Drafting of manuscript, acquisition and analysis of data, critical revision with important intellectual content.
DLP and XWJ: Analysis of data.
ALL AUTHORS: Approval of the final version of the manuscript to be published.
Author details
Zhou Xu1, Yunsong Lu1, Heng Li1, Dailiang Peng1, Xuwei Jiang1, Yubin Kou1
- Department of General Surgery, Shanghai Baoshan District Hospital of Integrated Traditional and Western Medicine, Shanghai, China
References
- Kristoffersen S, Normann SA, Morild I, Lilleng PK, Heltne JK. The hazard of sharp force injuries: factors influencing outcome. J Forensic Leg Med. 2016;37:71–7. https://doi.org/10.1016/j.jflm.2015.10.005
- Dittrich K, Abu-Zidan FM. Role of ultrasound in mass-casualty situations. Int J Disaster Med. 2004;2(1–2):18–23; https://doi.org/10.1080/15031430410024813
- Bokhari F, Nagy K, Roberts R, Brakenridge S, Smith R, Joseph K, et al. The ultra-sound screen for penetrating truncal trauma. Am Surg. 2004;70(4):316.
- Arumugam S, Al-Hassani A, El-Menyar A, Abdelrahman H, Parchani A, Peralta R, et al. Frequency, causes and pattern of abdominal trauma: a 4-year descriptive analysis. J Emerg Trauma Shock. 2015;8(4):193–8. https://doi.org/10.4103/0974-2700.166590
- Nishimura T, Sakata H, Yamada T, Terashima M, Shirai K, Yamada I, et al. Different patterns in abdominal stab wound in the self-inflicted and assaulted patients: an observational analysis of single center experience. Kobe J Med Sci. 2017;63(1):E17–21.
- Buzio M, Bertello A, Bau G, Mao P. Ultrasound in trauma (FAST). Minerva Chir. 2000;55(1–2):89–95. PMID: 10832291.
- Yıldız MK, Ozkan E, Odabaşı HM, Eriş C, Günay E, Abuoğlu HH, et al. Analysis of 120 patients with abdominal stab wound focusing on diagnostic role of fast. Int J Exp Med. 2014;7(5):1386–90.
- Lingawi SS, Buckley AR. Focused abdominal US in patients with trauma. Radiology. 2000;217(2):426–9. https://doi.org/10.1148/radiology.217.2.r00nv23426
- Mehta N, Babu S, Venugopal K. An experience with blunt abdominal trauma: evaluation, management and outcome. Clin Pract. 2014;4(2):34–7. https://doi.org/10.4081/cp.2014.599
- Como JJ, Bokhari F, Chiu WC, Duane TM, Holevar MR, Tandoh MA, et al. Practice management guidelines for selective nonoperative management of penetrating abdominal trauma. J Trauma. 2010;68(3):721–33. https://doi.org/10.1097/TA.0b013e3181cf7d07
- Siddharth BR, Keerthi MSS, Naidu SB, Venkanna M. Penetrating injuries to the abdomen: a single institutional experience with review of literature. Indian J Surg. 2017;79(3):196–200. https://doi.org/10.1007/s12262-016-1459-0
- Karamercan A, Yilmaz TU, Karamercan MA, Aytaç B. Blunt abdominal trauma: evaluation of diagnostic options and surgical outcomes. Ulus Travma Acil Cerrahi Derg. 2008;14(3):205.
- Qi X, Tian J, Sun R, Zhang H, Han J, Jin H, et al. Focused assessment with sonography in trauma for assessment of injury in military settings: a meta-analysis. Balkan Med J. 2020;37(1):3–8. https://doi.org/10.4274/balkanmedj.galenos.2019.2019.8.79
- Sheng AY, Dalziel P, Liteplo AS, Fagenholz P, Noble VE. Focused assessment with sonography in trauma and abdominal computed tomography utilization in adult trauma patients: trends over the last decade. Emerg Med Int. 2013;2013:678380. https://doi.org/10.1155/2013/678380
- Radwan RW, Tang AM, Beasley WD. Computed tomography as a first-line investigation for elderly patients admitted to a surgical assessment unit. Ann R Coll Surg Engl. 2018;100(4):285–9. https://doi.org/10.1308/rcsann.2017.0231
- Como JJ, Bokhari F, Chiu WC, Duane TM, Holevar MR, Tandoh MA, et al. Practice management guidelines for selective non-operative management of penetrating abdominal trauma. J Trauma Acute Care Surg. 2010;68(3):721–33. https://doi.org/10.1097/TA.0b013e3181cf7d07
- Biffl WL, Moore EE. Management guidelines for penetrating abdominal trauma. Curr Opin Crit Care. 2010;16(6):609–17. https://doi.org/10.1097/MCC.0b013e32833f52d2
- Scholz KH, Maier SKG, Maier LS, Lengenfelder B, Jacobshagen C, Jung J, et al. Impact of treatment delay on mortality in ST-segment elevation myocardial infarction (STEMI) patients presenting with and without haemodynamic instability: results from the German prospective, multicentre FITT-STEMI trial. Eur Heart J. 2018;39(13):1065–1074. https://doi.org/10.1093/eurheartj/ehy004
Keywords: Sharp force injury, Retrospective, Abdominal injury, Evaluation, Outcome, Complications.

Publication History
Received: March 26, 2021
Revised: May 17, 2021
Accepted: June 04, 2021
Published: June 30, 2021
Authors
Zhou Xu
Surgery Department, Shanghai Baoshan District Hospital of Integrated Traditional and Western Medicine, Shanghai - China.
Yunsong Lu
Surgery Department, Shanghai Baoshan District Hospital of Integrated Traditional and Western Medicine, Shanghai - China.
Heng Li
Surgery Department, Shanghai Baoshan District Hospital of Integrated Traditional and Western Medicine, Shanghai - China.
Dailiang Peng
Surgery Department, Shanghai Baoshan District Hospital of Integrated Traditional and Western Medicine, Shanghai - China.
Xuwei Jiang
Surgery Department, Shanghai Baoshan District Hospital of Integrated Traditional and Western Medicine, Shanghai - China.
Yubin Kou
Surgery Department, Shanghai Baoshan District Hospital of Integrated Traditional and Western Medicine, Shanghai - China.