Original Article
Volume: 39 | Issue: 1 | Published: Mar 26, 2023 | Pages: 25 - 32 | DOI: 10.24911/BioMedica/5-683
Determinants of Parental Knowledge and Attitude towards Poliomyelitis and its Immunization in Sialkot city: A Mix Method Study
Authors:
Taskeen Zahra
, Ayesha Parvez
, Hamza Ahmad
, Hassiba Ifftikhar
, Faisal Mushtaq
![]() , Saima Ayub
, Saima Ayub
Article Info
Authors
Taskeen Zahra
Associate Professor, Department of Community Medicine, Fatima Jinnah Medical University, Lahore, Pakistan.
Ayesha Parvez
Ph.D. Sch. , Department of Public Health, Institute of Social and Cultural Sciences, University of the Punjab, Lahore, Pakistan.
Hamza Ahmad
MBBS Student, Khawaja Muhammad Safdar Medical College, Sialkot, Pakistan.
Hassiba Ifftikhar
MBBS Student, Khawaja Muhammad Safdar Medical College, Sialkot, Pakistan.
Faisal Mushtaq
Demonstrator, Department of Biostatistics, Institute of Public Health, Lahore, Pakistan.
Saima Ayub
Institute of Public Health, Lahore, Pakistan.
Publication History
Received: August 25, 2022
Accepted: February 15, 2023
Published: March 26, 2023
Abstract
Background and Objectives: Poliomyelitis still remains a significant public health concern in developing countries though it has been eradicated from most of the world. Illiteracy, cultural constraints, and skepticism of the general public regarding vaccination are considered major impediments to its successful eradication from developing countries. In this study, the authors aimed to evaluate parental knowledge and attitudes about poliomyelitis and its immunization in a local population as well as to elucidate the determinants and barriers relating to the immunization process.
Methods: This mixed-method study was conducted on 350 consenting parents who accompanied their children under 5 years of age at the pediatric outdoors of a tertiary care hospital in Sialkot, Pakistan. Parents of only those children were included for the study who had failed to receive a polio dose during the last two supplementary immunization activities The parents were interviewed on a pre-tested, semi structured questionnaire. Statistical Package for the Social Sciences was used for statistical analysis considering p-value <0.05 as significant.
Results: Among 350 parents, 91.7% lacked knowledge about polio vaccination and 82% reported a negative attitude towards the disease and its immunization. A total of 11.4% of subjects completely refused to get their child vaccinated. The socioeconomic status, religious myths, level of literacy, and occupation of the parents significantly influenced their level of knowledge and attitude toward the disease and its vaccination (p < 0.05).
Conclusion: Poor knowledge and negative attitudes of parents towards poliomyelitis vaccination were observed. Fear of side effects and religious beliefs were identified as the most common barriers to immunization toward achieving polio eradication.
Keywords: parents, knowledge, attitude, polio, polio vaccine, barriers

Biomedica - Official Journal of University of Health Sciences, Lahore, Pakistan
Volume 39(1):25-32
ORIGINAL ARTICLE
Determinants of parental knowledge and attitude towards poliomyelitis and its immunization in Sialkot city: a mix method study
Taskeen Zahra1*, Ayesha Parvez2, Hamza Ahmad3, Hassiba Iftikhar3, Faisal Mushtaq4, Saima Ayub5
Received: 25 August 2022 Revised date: 28 December 2023 Accepted: 15 February 2023
Correspondence to: Taskeen Zahra
*Associate Professor, Department of Community Medicine, Fatima Jinnah Medical University, Lahore, Pakistan.
Email: dr.taskeenzahra@yahoo.com
Full list of author information is available at the end of the article.
ABSTRACT
Background and Objectives:
Poliomyelitis still remains a significant public health concern in developing countries though it has been eradicated from most of the world. Illiteracy, cultural constraints, and skepticism of the general public regarding vaccination are considered major impediments to its successful eradication from developing countries. In this study, the authors aimed to evaluate parental knowledge and attitudes about poliomyelitis and its immunization in a local population as well as to elucidate the determinants and barriers relating to the immunization process.
Methods:
This mixed-method study was conducted on 350 consenting parents who accompanied their children under 5 years of age at the pediatric outdoors of a tertiary care hospital in Sialkot, Pakistan. Parents of only those children were included for the study who had failed to receive a polio dose during the last two supplementary immunization activities The parents were interviewed on a pre-tested, semi-structured questionnaire. Statistical Package for the Social Sciences was used for statistical analysis considering p-value <0.05 as significant.
Results:
Among 350 parents, 91.7% lacked knowledge about polio vaccination and 82% reported a negative attitude towards the disease and its immunization. A total of 11.4% of subjects completely refused to get their child vaccinated. The socioeconomic status, religious myths, level of literacy, and occupation of the parents significantly influenced their level of knowledge and attitude toward the disease and its vaccination (p < 0.05).
Conclusion:
Poor knowledge and negative attitudes of parents towards poliomyelitis vaccination were observed. Fear of side effects and religious beliefs were identified as the most common barriers to immunization toward achieving polio eradication.
Keywords:
Parents, knowledge, attitude, polio, vaccine, barriers, eradication.
Introduction
There has been a polio eradication campaign and initiative in Pakistan for more than 25 years; however, the country is still far away from achieving its goal of ending polio in this part of the world.1 Polio vaccines, oral and injectable, contributed to the eradication of the disease, and gains were made globally against the disease through stronger immunization programs. However, missed opportunities to vaccinate children during vaccination drives are becoming increasingly catastrophic for the eradication of polio in Pakistan.1-3 The vaccination drives in Pakistan are still not reaching a large number of children despite efforts such as recruiting female community workers and interacting with Afghan authorities at border areas.4
World Health Organization (WHO) considers vaccine hesitancy as one of the top 10 health threats in the world, manifesting in refusal to vaccinate in both developed and developing/transitional countries.5 In Pakistan, refusal rates to polio vaccination vary from as low as 3.15% in Islamabad and Rawalpindi regions6, to 8.1% in Quetta7, 27.9% in Bannu District8, and 61.3% in Karachi.9
Vaccination provides substantial benefits by reducing disease, disability, and death and enhancing herd immunity as a reduction of mortality and morbidity in children under the age of 5.1 Religious beliefs and dogmas greatly influence human behavior, particularly in healthcare. In Pakistan, the polio vaccination campaign and its mass campaigns are under fire, which impedes the achievement of targets to end the situation of endemic polio.10
Low maternal literacy rates and human development index, a geo-political situation with misconceptions and a lack of awareness about the polio vaccine are major barriers besides many flaws in the health care as well as the political system. Approximately 250,000 children living in Khyber Pakhtunkhwa province of Pakistan are at risk of contracting polio due to resistance to vaccination, which is attributed to a number of factors, including inaccessibility to certain geographical areas, security threats to vaccination teams, a lack of female vaccine providers, and refusal to receive vaccination.10,11
A periodic evaluation of the knowledge and attitudes of the concerned community is inevitable because it assists in the design of data-driven interventions to change the attitudes.
Taking into account the conclusions published by the local studies regarding knowledge and attitude towards polio and its immunization, this research was carried out among residents of the Sialkot City of Pakistan regarding polio vaccination to help us understand the currently prevailing factors that are driving the polio vaccination acceptance and success in Pakistan. Sialkot, with a literacy rate of 59%, is located far from developed cities such as Lahore, and is close to the border, putting it in a status in which the gaps in knowledge and attitude of residents regarding polio vaccination and exploring the barriers pertaining to them can be identified to address these factors for the ultimate elimination of this disease from Pakistan.
Methods
This descriptive mixed method study was conducted at the Khawaja Muhammad Safdar Medical College, Sialkot District of Punjab, Pakistan from April to June 2018 after taking approval from the Institutional Ethical Board. An estimated sample size of 350 parents was determined using the WHO sample size calculator (2.0) considering the attrition and refusal rates of 10% (WU1) and the expected probability of previous similar studies.6
Parents accompanying children under 5 years of age who had failed to receive or refused to get administered a polio dose during the last two supplementary immunization activities were randomly enrolled in the study through systematic sampling in the pediatric outpatient department of the said hospital. The first parent accompanying her/his child was selected randomly from the outdoor register and then every 8th was approached to participate in the study. Parents of children already diagnosed with poliomyelitis, suffering from chronic illness, autoimmune diseases, or paralysis other than polio, and who were unwilling to participate were excluded.
A pre-tested, semi-structured questionnaire consisting of three sections was used to interview the selected population. Section A of the questionnaire was about the socio-demographic profile while sections B and C depicted the knowledge and attitude toward polio immunization. The data obtained from section A was categorized according to the available statistics from a local registry of Pakistan.12 The knowledge and attitude of parents were assessed through a closed-ended questionnaire (Section-B) after their consent was obtained.
A pre-test was conducted on 20 parents by trained data collectors, whose results were not included in the final analysis of the questionnaire. The questionnaire was validated for both content and face validity. Based on the recommendations of the data collectors, necessary changes were made.
Data collection lasted 5 weeks, 6 days a week, with an average of eight interviews done per day. The interviews were conducted at the same pace and duration in order to minimize inter-rater bias.
A total of 12 questions were designed as part of the knowledge section, with one score being given for each correct answer. A score of less than 80% was considered inadequate and a score of more than 80% was considered adequate. Eight attitude questions were asked and responses were scored based on a 5-point Likert scale ranging from strongly disagree to strongly agree. An attitude score of 80% (32/40) was taken as negative.13
A total of 40 enrolled parents who completely refused to get their children vaccinated were selected for an in-depth interview in order to identify the underlying barriers. A female researcher initially contacted the parents by telephone to explain the purpose of the call and obtain their consent for the interview. In case of the female respondent, the assurance call was extended to her male partner and a follow-up appointment was scheduled. Telephonic in-depth interviews were conducted at the agreed time, and the interviews were recorded on the same device after informed consent was taken from the parents.
Statistical analysis
Statistical Package for the Social Sciences version 23.0 was used for data entry and analysis. Percentage and frequencies were determined for qualitative variables, like gender while mean and SD were calculated for quantitative variables like age, knowledge, and attitude. For determinants, the socio-demographic profile of the parents was taken into account. Socioeconomic status was categorized as people having monthly incomes <50,000 and >50,000. Chi-square test was used as a test of significance and p value of <0.05 was considered statistically significant.
Results
The study showed that the mean age of the accompanying parent was 28.38 ± 23.63 years whereas 191 (54.5%) out of 350 were ≤24 years and 159 (45.5%) had age >24 years.
Among 350 children, 241 (68.9%) were males and 109 (31.1%) were females, with 170 (48.5%) living in urban areas and 180 (51.5%) living in rural areas.
Data from Section A of the questionnaire12 revealed that there were 312 (89.1%) parents with an income ≤50,000 rupees with a mean income of Rs. 38,380 ± 62,373 for all the subjects. A total of 179 (51.1%) parents were illiterate while 306 (87.4%) were skilled and involved in one or another kind of labor/job (Table 1).
Out of 350 children, a reasonable number [310 (88.6%)] of children were vaccinated among which 125 (40.3%) had extended program on immunization cards available to them. While analyzing the trend of punctuality for vaccinations, 278 (89.6%) parents were found to comply with the scheduled vaccination calendar for their child. Among all the respondents, the overall mean knowledge score was found as 6.20 ± 2.51, and mean attitude score was 17.8 ± 2.86 (Figure 1).
Among the respondents with age 24 years, 6.8% were found to have adequate knowledge regarding polio and its vaccination, whereas 10% had sufficient knowledge at age >24 years. (p = 0.331) (Table 1).
According to the gender variation, 9.5% of males and 5.5% of females had adequate knowledge (p = 0.294). Based on the effect of residence type on level of knowledge, 12.7% of parents from urban areas had adequate knowledge as opposed to 0.5% of parents from rural areas (p = 0.031).
Financial status showed that 18% of parents with income >50,000 rupees had adequate knowledge (p = 0.026). A total of 20 (11.7%) literate and 21 (7.1%) skilled fathers had adequate knowledge regarding the disease and its vaccination (p = 0.03; p = 0.018) (Table 1).
The association between age and level of parental attitude showed no significant association (p = 0.667). Among 350 parents, 50 (29.2%) literate fathers and 61 (20.1%) skilled fathers exhibited positive attitudes (p = 0.001; p = 0.01) (Table 2).
Table 1. Association of socio-demographic profile with the parental knowledge about polio and its vaccination (n = 350).
| Characteristics | Knowledge | Total | p-value | |
|---|---|---|---|---|
| Adequate** frequency (%) | Inadequate frequency (%) | |||
| Age in years | ||||
| ≤24 | 13 (6.8) | 178 (93.2) | 191 (100) | 0.331 |
| >24 | 16 (10.0) | 143 (90.0) | 159 (100) | |
| Total | 29 (8.3) | 321 (91.7) | 350 (100) | |
| Gender | ||||
| Male | 23 (9.5) | 218 (90.4) | 241 (100) | 0.294 |
| Female | 6 (5.5) | 103 (94.5) | 109 (100) | |
| Total | 29 (8.3) | 321 (91.7) | 350 (100) | |
| Residence | ||||
| Urban | 20 (11.7) | 150 (88.3) | 170 (100) | 0.031* |
| Rural | 9 (0.5) | 171 (99.5) | 180 (100) | |
| Total | 29 (8.3) | 321 (91.7) | 350 (100) | |
| Income in PKR/Month | ||||
| ≤50,000 | 22 (7.0) | 290 (93.0) | 312 (100) | 0.026* |
| >50,000 | 7 (18.4) | 31 (81.6) | 38 (100) | |
| Total | 29 (8.3) | 321 (91.7) | 350 (100) | |
| Father education | ||||
| Literate | 20 (11.7) | 151 (88.3) | 171 (100) | 0.031* |
| Illiterate | 9 (5) | 170 (95) | 179 (100) | |
| Total | 29 (8.3) | 321 (91.7) | 350 (100) | |
| Child’s father's occupation | ||||
| Skilled | 21 (7) | 285 (93) | 306 (100) | 0.018* |
| Unskilled | 8 (18) | 36 (82) | 44 (100) | |
| Total | 29 (8.2) | 321 (91.7) | 350 (100) | |
*Chi-square test p value <0.05 taken as significant; **Adequate knowledge: Score ≥10 out of 12 on questionnaire.
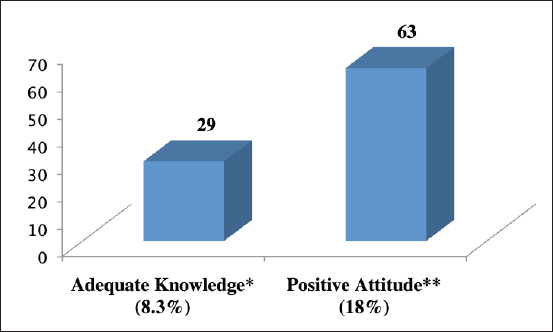
Figure 1. Parent’s knowledge and attitude towards poliomyelitis and its immunization (n = 350). *Adequate knowledge: >10 out of 12; **Positive attitude: score ≤32 out of 40.
Table 2. Association of socio-demographic profile with the parental attitude towards polio and its immunization (n = 350).
| Characteristics | Attitude | Total | p-value | |
|---|---|---|---|---|
| Positive** frequency (%) | Negative frequency (%) | |||
| Age in years | ||||
| ≤24 | 36 (18.8) | 155 (81.2) | 191 (100) | 0.677 |
| >24 | 27 (16.9) | 132 (83.1) | 159 (100) | |
| Total | 63 (18) | 287 (82) | 350 (100) | |
| Gender | ||||
| Male | 46 (20.3) | 195 (79.7) | 241 (100) | 0.457 |
| Female | 17 (15.5) | 92 (84.5) | 109 (100) | |
| Total | 63 (18) | 287 (82) | 350 (100) | |
| Type of residence | ||||
| Urban | 40 (23.5) | 130 (76.5) | 170 (100) | 0.011* |
| Rural | 23 (12.7) | 157 (87.3) | 180 (100) | |
| Total | 63 (18) | 287 (82) | 350 (100) | |
| Income in PKR/Month | ||||
| ≤50,000 | 58 (18.5) | 254 (81.5) | 312 (100) | 0.507 |
| >50,000 | 5 (13.1) | 33 (86.9) | 38 (100) | |
| Total | 63 (18) | 287 (82) | 350 (100) | |
| Father education | ||||
| Literate | 50 (29.2) | 141 (70.8) | 171 (100) | <0.001* |
| Illiterate | 13 (7.2) | 146 (92.8) | 179 (100) | |
| Total | 63 (18) | 287 (82) | 350 (100) | |
| Father occupation | ||||
| Skilled | 61 (20) | 245 (80) | 306 (100) | 0.010* |
| Unskilled | 2 (7.0) | 42 (93) | 44 (100) | |
| Total | 63 (18) | 287 (82) | 350 (100) | |
*Chi-square test p-value <0.05 taken as significant; **Positive attitude: score ≤32 out of 40 on questionnaire.
During the in-depth interviews, the following themes were identified as barrier factors against immunization: a) fear of side effects, b) religious reasons, c) non-compliant family members, d) lack of knowledge, e) conspiracy and political agenda of the West, f) distrust on the government vaccines, g) security concerns, and h) myths and misconceptions like infertility, loss of potency among male children, etc., also identified (Figure 2).
Discussion
Many factors influence the decision of parents regarding their children’s vaccine including, but not limited to, inadequate knowledge and perception, misleading information, and strong anti-vaccination campaigns for political agendas.14
The present study reports a mean score of parental knowledge regarding polio and its vaccination as 6.20 + 2.5 and a parental attitude score of 17.8 + 2.86. A study conducted by Mirani et al.15 revealed that most guardians and parents in Gadap Town, Karachi, Pakistan were aware of polio and recognized it as a public health concern. Khan et al.11 in their two subsequent studies from Quetta and Peshawar cities of Pakistan reported 38.8% of participants had good knowledge about polio with a mean knowledge score of 7.35 ± 2.54 while a significant proportion of the participants had negative attitudes toward polio vaccination (84.8%), with a mean score of 19.2 ± 2.39.16
Nanbur et al.17 reported in their non-experimental descriptive study of Nigerian mothers that the majority (84.3%) had knowledge of poliomyelitis; 94.3% were aware of the polio vaccine; and, furthermore, it was determined that mothers who knew about poliomyelitis were more likely to accept vaccination for their children (p < 0.05). This study clearly demonstrated that increasing the public’s awareness of polio and its vaccine would be an effective method of eradicating polio.
It was found that urban residence, level of education of both parents, higher income, and having a skilled job, were associated with adequate knowledge (p < 0.05). Parents with higher incomes have greater access to knowledge and vaccinations as reported by Shafique et al.18 from another study from Pakistan.
Unlike the findings of Khan et al.11 where younger participants appeared to have a higher level of knowledge than the older ones, no such relation was found in the present study. Knowledge about polio and its immunization is also lower among parents with low incomes, informal education, and those living in rural areas.17 Vaccination coverage in Pakistan is reported to be below global standards. For example, coverage for the bacillus Calmette-Guerin vaccine for tuberculosis is reported to be 80%, while it is much lower, 60% and 67%, respectively for polio and measles vaccination. There are many factors contributing to this disparity including logistical barriers, inadequately trained healthcare personnel, insufficient parental awareness and education as well as the business, religious, and politics-related influences on vaccine marketing.19
The present study did not find any association between knowledge regarding polio and its immunization and the gender of the parents. The results of this study are concordant with the findings of Shafique et al.18 However, Khan et al.20 found that poor uptake of polio vaccines was associated with illiteracy, socioeconomic status, and women empowerment.
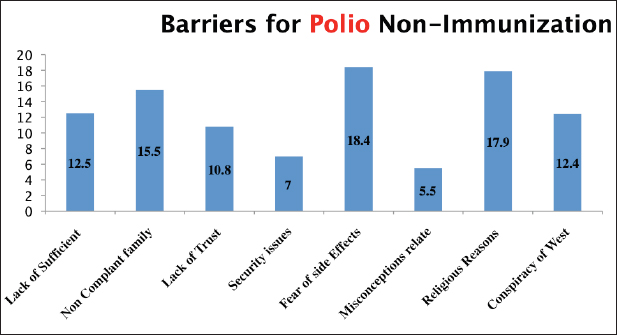
Figure 2. The bar chart shows the barriers to polio vaccination as identified by 40 respondents who refused to get their children vaccinated.
In the current study, a positive association of knowledge and attitude with the skilled occupation of fathers (p value 0.01 and 0.018, respectively) was observed. Merani et al.15 and Khan et al.16 found that fathers with private jobs were more knowledgeable about polio vaccinations.
Regarding attitude, the present study showed a positive attitude toward the polio vaccine with a mean score of 17.8 + 2.86 in 18% of respondents. The positive attitude was found to be related to urban dwellers, those having better education and skillful occupation. Similar findings were reported by Khan et al.,11 who found that most of (84.8%) their respondents had a negative attitude, with a mean score of 19.19 ± 2.39. Moreover, they found that a rural setting and a lack of education contributed to negative attitudes. There was however no evidence found for an association between economic status and attitude of subjects towards polio and its immunization.15
Several barriers to polio immunization have been identified in the present study including lack of knowledge, non-compliant family members and/or spouses, lack of trust in the government vaccine, security concerns, a misconception that the vaccine causes infertility, religious beliefs that the contents are haram, as well as political agendas of the west and conspiracy theories.
There is a lack of trust in the quality of the vaccine, as well as doubts about maintaining the cold chain temperature. There was a concern among parents as the ability of the government to maintain a cold chain in times of frequent power interruptions and concern over the gadgets and equipment used by the healthcare workers during their door-to-door campaigns in extreme weather conditions.21,22
It has been found that in order to address the issue of polio vaccine refusal, local values as well as cultural, religious, and political factors must be addressed.22,23 Khan et al.11 identified similar results with religious beliefs (39.06%), inadequate knowledge (33.7%), and fear of infertility by polio vaccines (32.16%) and security issues (29.42%) as major reported barriers.
Regardless of the situation, misinformation and negative attitudes toward the polio vaccine manifest themselves as hostility and security threats to those working on the polio epidemic.24 It was found by Verma et al.24 from India that polio was 73% more prevalent during insecure conditions (95% confidence interval: 30%-131%) in comparison to secure geographical areas.
In our study, 40 children were never vaccinated which shows the sheer momentum of the “missed children” during polio campaigns. According to our findings and other reported literature, transferring knowledge from trusted sources such as religious and community leaders, as well as incorporating group-influence techniques into advocacy can be of great assistance in overcoming barriers and parental hesitancy towards polio immunization.25
The result of this study will help the stakeholders to evaluate the effectiveness of their policies regarding the eradication of polio from Pakistan. The insight gained can contribute to highlighting the individual and contextual aspects of polio immunization and its barriers. The results of this study may not be generalizable, therefore precautionary measures should be taken when interpreting the findings. Because participation in this study was voluntary, we cannot disregard the possibility of self-selection bias by participants who are more concerned with polio.
Conclusion
Immunization coverage and its compliance are crucial for preventing and eradicating poliovirus infections in Pakistan. Adequate parental knowledge while addressing the barriers like fear of side effects, religious beliefs, and mistrust about the health safety of the vaccines, can bring about a positive change in the attitude of parents towards immunization against this disease.
Limitations of the study
The study has many limitations. Firstly, the resource constraints in the form of time, money, material, and expertise were inevitable. As it was a non-funded study, the incentive other than travel allowance to a handful of the parents, couldn’t be given, hence telephonic interviews were conducted. A better community-based research study design involving all ethnicities; the larger group would have given a clear understanding of the issue. Parental refusal was more than expected and it might have been more with a larger sample size hence the results of the study from a single center may not be generalizable.
Acknowledgement
The authors acknowledge Dr. Noreen Maqbool Bukhari, Head Department of Community Medicine, Khawaja Muhammad Safdar Medical College, Sialkot, Pakistan, for her support during the execution of this research. The study would have not been possible without the help of Department of Community Medicine at Khawaja Muhammad Safdar Medical College, Sialkot, Pakistan.
List of Abbreviations
| WHO | World Health Organization |
Conflict of interest
None to declare.
Grant support and financial disclosure
None to disclose.
Ethical approval
Ethical approval was granted by the Institutional Ethics Committee of Government Khawaja Safdar Medical College Sialkot, Pakistan, vide Letter No. 30/REC/KMSMC dated 18-08-2018.
Authors’ contributions
TZ: Conception and design of study, drafting of manuscript with critical intellectual input.
AP; HI; FM: Acquisition and analysis of data, drafting of the manuscript
HA: Acquisition and analysis of data
SA: Drafting of the manuscript with critical intellectual input.
ALL AUTHORS: Approval of the final version of the manuscript to be published.
Authors’ Details
Taskeen Zahra1, Ayesha Parvez2, Hamza Ahmad3, Hassiba Iftikhar3, Faisal Mushtaq4, Saima Ayub5
- Associate Professor, Department of Community Medicine, Fatima Jinnah Medical University, Lahore, Pakistan
- Ph. D Scholar, Department of Public Health, Institute of Social and Cultural Sciences, University of the Punjab, Lahore, Pakistan
- MBBS Student, Khawaja Muhammad Safdar Medical College, Sialkot, Pakistan
- Demonstrator, Department of Biostatistics, Institute of Public Health, Lahore, Pakistan
- Institute of Public Health, Lahore, Pakistan
References
- Shabbir H, Saeed S, Farhan M, Abbas K, Rehman ME, Gul F, et al. Poliomyelitis in Pakistan: challenges to polio eradication and future prospects. Ann Med Surg (Lond). 2022;80:104274. https://doi.org/10.1016/j.amsu.2022.104274
- GPEI-Pakistan [Internet]. Polioeradication.org. 2020 [cited 2020 Nov]. Available from: https://polioeradication.org/where-we-work/pakistan/
- Polio Cases Update 2020 Across Pakistan’s Provinces [Internet]. Endpolio.com.pk. 2020 [cited 2020 Nov]. Available from: https://www.endpolio.com.pk/polioin-pakistan/polio-cases-in-provinces
- Pakistan Polio Eradication Initiative National Emergency Action Plan 2021-2023 [Internet]. Pakistan polio eradication initiative national emergency action plan. Islamabad, Pakistan: National Emergency Operation Centre. [cited 2020 Oct]. Available from: https://polioeradication.org/wp-content/uploads/2022/02/NEAP-2021-2023.pdf
- Bussink-Voorend D, Hautvast JL, Vandeberg L, Visser O, Hulscher ME. A systematic literature review to clarify the concept of vaccine hesitancy. Nat Hum Behav. 2022;6(12):1634–48. https://doi.org/10.1038/s41562-022-01431-6
- Hussain A, Zahid A, Malik M, Ansari M, Vaismoradi M, Aslam A, et al. Assessment of parents’ perceptions of childhood immunization: a cross-sectional study from Pakistan. Children (Basel). 2021;8(11):1007. https://doi.org/10.3390/children8111007
- Zarak MS, Sana H, Arshad Z, Saleem A, Shah M, Tareen H, et al. Understanding the reasons for refusal of polio vaccine by families in Quetta Block, Pakistan. East Mediterr Health J. 2022;28(7):498–505. https://doi.org/10.26719/emhj.22.052
- Khattak FA, Rehman K, Shahzad M, Arif N, Ullah N, Kibria Z, et al. Prevalence of parental refusal rate and its associated factors in routine immunization by using WHO vaccine hesitancy tool: a cross sectional study at district Bannu, KP, Pakistan. Int J Infect Dis. 2021;104:117–24. https://doi.org/10.1016/j.ijid.2020.12.029
- Khaliq A, Elahi AA, Zahid A, Lassi ZS. A survey exploring reasons behind immunization refusal among the parents and caregivers of children under two years living in urban slums of Karachi, Pakistan. Int J Environ Res Public Health. 2022;19(18):11631. https://doi.org/10.3390/ijerph191811631
- Basharat S, Shaikh BT. Polio immunization in Pakistan: ethical issues and challenges [Internet]. Public Health Rev. 2017;38(1):6. https://doi.org/10.1186/s40985-017-0049-4
- Khan MU, Ahmad A, Salman S, Ayub M, Aqeel T, Haq NU, et al. Muslim scholars’ knowledge, attitudes and perceived barriers towards polio immunization in Pakistan. J Relig Health. 2017;56(2):635–48. https://doi.org/10.1007/s10943-016-0308-6
- Pakistan Bureau of Statistics. District Report, Sialkot. Islamabad, Pakistan: Government of Pakistan; 2020.
- Maung TM, Kulandaivalu S, Xian CM, Ramachandra K, Jai Devaraj S, Venkadason T, et al. Knowledge, attitude, and barriers toward polio immunization among pre-clinical students in Malaysia. Asian J Med Sci. 2021;12(11):53–9. https://doi.org/10.3126/ajms.v12i11.38462
- Vezzosi L, Santagati G, Angelillo IF. Knowledge, attitudes, and behaviors of parents towards varicella and its vaccination. BMC Infect Dis. 2017;17(1):172. https://doi.org/10.1186/s12879-017-2247-6
- Mirani A, Holakouie-Naieni K, Majdzadeh R, Nematollahi S, Baig S. Knowledge, attitude, and practices about polio vaccination of the guardian in super high-risk areas of Gadap town, Karachi, Pakistan. Iran J Public Health. 2017;46(5):715–6.
- Khan MU, Ahmad A, Aqeel T, Salman S, Ibrahim Q, Idrees J, et al. Knowledge, attitudes and perceptions towards polio immunization among residents of two highly affected regions of Pakistan. BMC Public Health. 2015;15(1):1100. https://doi.org/10.1186/s12889-015-2471-1
- Nanbur S, Yimi S, Joseph GP, Nanim N. Knowledge, attitude and practice of mothers towards the acceptance of oral polio vaccine for their children in Mista-Ali community, JOS, Plateau state, Nigeria. Int J Med Health Res. 2019;5(5):95–101.
- Shafique F, Hassan MU, Nayab H, Asim N, Akbar N, Shafi N, et al. Attitude and perception towards vaccination against poliomyelitis in Peshawar, Pakistan. Rev Saude Publica. 2021;55(55):104. https://doi.org/10.11606/s1518-8787.2021055003478
- Butt M, Mohammed R, Butt E, Butt S, Xiang J. Why have immunization efforts in Pakistan failed to achieve global standards of vaccination uptake and infectious disease control? Risk Manag Healthc Policy. 2020;13:111–24. https://doi.org/10.2147/RMHP.S211170
- Khan MT, Zaheer S, Shafique K. Maternal education, empowerment, economic status and child polio vaccination uptake in Pakistan: a population based cross sectional study. BMJ Open. 2017;7(3):e013853. https://doi.org/10.1136/bmjopen-2016-013853
- Andrade GE, Hussain A. Polio in Pakistan: political, sociological, and epidemiological factors. Cureus. 2018;10(10):e3502. https://doi.org/10.7759/cureus.3502
- Shah SF, Ginossar T, Weiss D. This is a Pakhtun disease: Pakhtun health journalists’ perceptions of the barriers and facilitators to polio vaccine acceptance among the high-risk Pakhtun community in Pakistan. Vaccine. 2019;37(28):3694–703. https://doi.org/10.1016/j.vaccine.2019.05.029
- Jamal D, Zaidi S, Husain S, Orr DW, Riaz A, Farrukhi AA, et al. Low vaccination in rural Sindh, Pakistan: a case of refusal, ignorance or access? Vaccine. 2020;38(30):4747–54. https://doi.org/10.1016/j.vaccine.2020.05.018
- Verma AA, Jimenez MP, Tangermann RH, Subramanian SV, Razak F. Insecurity, polio vaccination rates, and polio incidence in northwest Pakistan. Proc Natl Acad Sci USA. 2018;115(7):1593–8. https://doi.org/10.1073/pnas.1711923115
- Saleh W, Jami H. Group influence on attitudes towards polio vaccination in Pakistan: role of group identification and perceived group support for polio vaccines. J Pak Med Assoc. 2022;72(5):802–6. https://doi.org/10.47391/JPMA.3238