Biomedica - Official Journal of University of Health Sciences, Lahore, Pakistan
Volume 40(2):100-106
ORIGINAL ARTICLE
Practices of dental care and treatment provided to pediatric patients in private dental clinics in Lahore, Pakistan
Memoona Javed1, Amjad H Wyne2, Hammad Hassan3*
Received: 03 March 2024 Revised date: 20 May 2024 Accepted: 14 June 2024
Correspondence to: Hammad Hassan
*Department of Science of Dental Materials, University of Health Sciences, Lahore, Pakistan.
Email: hammadhassanh@gmail.com
Full list of author information is available at the end of the article.
ABSTRACT
Background and Objective:
With the high prevalence of dental caries among children in Pakistan and the limited availability of pediatric dentists, dental care is provided majorly by general dentists. This study aims to determine the preventive dental care provided to pediatric dental patients by general dentists in private practice settings in Lahore.
Methods:
This cross-sectional study was conducted among 185 general dentists working in private dental clinics in Lahore, utilizing an online validated questionnaire designed by the authors and distributed through email and WhatsApp using a purposive sampling technique. Data were analyzed using statistical software, and p-value of 0.05 was taken as significant.
Results:
Most respondents (73.5%) reported the unavailability of pediatric dentists in their clinics. About one-third of the respondents always chose to refer their child to a pediatric dentist. About 48.1% of the general dentists were “somewhat aware” of the behavioral management techniques. Pediatric-specific dental treatment services were more frequently provided in clinics where a pediatric dentist was available. Fillings were the most frequent (90.8%) treatment services, along with extractions (79.5%), pulpectomies (69.2%), and pulpotomies (65.9%). Notably, 74.1% of the general dentists had not attended any workshop or course in pediatric dentistry.
Conclusion:
General dentists in private practices provide minimal dental treatment to pediatric patients, with a significant number lacking formal training in pediatric dentistry. This highlights the need for formal training programs to improve the quality of pediatric dental care.
Keywords:
Dental care, general dentists, pediatric dentistry, dental treatment.
Introduction
The provision of preventive dental care and treatment services to pediatric patients by general dentists in private practices is crucial, especially in regions like Lahore, Pakistan, where the prevalence of dental caries among children is significantly high.1,2 Oral diseases are common worldwide, with dental caries considered one of the most prevalent chronic diseases among children.3,4 Due to the high prevalence, the role of general dentists in private practices becomes even more critical. Pediatric dental practices, including preventive care, treatment services, and behavioral management techniques, are essential to combat the widespread issue of dental caries.2,5
Oral health care providers in many developing countries are more focused on the restorative aspect of dental diseases and are unable to control rapidly spreading dental diseases.6 Pediatric dentists play a vital role in providing high-quality dental health care to their patients, from birth to infancy to adolescence.7. Globally, pediatric dentistry is a well-established specialty with dedicated training programs and certifications. Countries like the United States (US) and the United Kingdom (UK) have a robust infrastructure for pediatric dental care.8,9 In the US, the American Academy of Pediatric Dentistry (AAPD) sets guidelines for pediatric dental care and offers board certification for specialists where dentists undergo rigorous training, including a residency program that focuses on child psychology, growth and development, and specialized clinical techniques.10 In the UK, the British Society of Pediatric Dentistry promotes education, research, and best practices in the field and dentists must complete a specialty training program and achieve certification from the General Dental Council.11
The number of trained pediatric dentists is very low in Pakistan, which means that general dentists have to provide dental treatment to pediatric dental patients.2,12 There are a limited number of pediatric dentists working in Lahore, which has a population of 9 million, with 34% of children below the age of 16.13 Therefore, the responsibility of providing dental care to these pediatric dental patients rests on the shoulders of the general dentists.2
This study aimed to assess the dental care and treatment services provided to children by general dentists in Lahore, the capital city of Punjab province in Pakistan. It also explored the use of distraction techniques and the dentists’ willingness to attend pediatric dentistry workshops and courses.
Methods
The questionnaire-based descriptive cross-sectional study was conducted from December 13, 2022, to July 1, 2023, among the general dentists working in leading private dental practices in Lahore Pakistan after taking approval from the Institutional Review Board of Institute of Dentistry, Combined Military Hospital, and Medical College, Lahore, Pakistan. The questionnaire was developed after an extensive literature review. The questionnaire underwent several revisions to make it more comprehensible for the respondents and was later validated through test re-test (in terms of content and face validity). The value of Cronbach’s alpha was 0.615, falling within the acceptable range. The questionnaire consisted of 16 close-ended questions. The first section of the questionnaire obtained demographic information about the participants, whereas the second section included questions about the extent of pediatric dental services provided by the dentists, the use of distraction techniques, and willingness to attend workshops and courses on pediatric dentistry. With 95% power of the study and a 5% level of significance, a total sample size of 185 participants was calculated through the non-probability purposive sampling technique.8 Data were collected through Google Forms (a GISD-approved and supported tool). The general dentists working in private practices were approached through email and WhatsApp and were requested to complete the questionnaire. Repeated reminders were given to ensure a higher response. The statements of consent and confidentiality were included in the questionnaire.
Statistical Analysis
Data were analyzed using IBM Statistical Package for Social Sciences (SPSS version 24, IBM Corporation, USA, New York, 2011). Various frequencies were generated. The chi-square test was used to determine associations between the categorical variables i.e., gender-wise comparison of distraction techniques and availability of visiting pediatric dentist. A p-value of equal to or less than 0.05 was set as significant.
Results
A total of 191 questionnaires were distributed, of which 185 participants responded, thus meeting the required sample size with a response rate of 97%. The demographic information of the participants is presented in Table 1.
The frequency of dental treatment provided to pediatric dental patients, their referral to a pediatric dentist, and the provision of preventive dental care by general dentists are illustrated in Figure 1. Most (56.2%) of the general dentists “sometimes” treated their pediatric patients. In the case of uncooperative pediatric patients, around one-third (35.7%) of the respondents always chose to refer the patient to a pediatric dentist.
The awareness of general dentists about behavioral management techniques, distraction techniques, and tooth eruption sequence is presented in Figure 2.
Toys (60.5%), restraints (50.8%), and auditory distractions (50.3%) were the top three frequently used distraction techniques (Table 2). The least (14.1%) utilized technique was virtual reality glasses (VR). The use of distraction techniques such as visual (distraction), VR glasses, and needle disguise were significantly (p < 0.05) more common in the female general dentists than the males. The use of physical restraints and toys was significantly (p < 0.05) higher in male dentists than in females (Table 2).
The various preventive dental services offered to pediatric dental patients by the general dentist are presented in Figure 3. Oral hygiene instructions (94.1%) and dietary advice (79.5%) were the most common services provided.
Table 3 compares the services provided to pediatric dental patients in terms of the availability/non-availability of a pediatric dentist in private practices. All the treatment modalities specific to trained pediatric dentists were seldom provided in those private practices where a visiting pediatric dentist was unavailable.
About two-thirds (74.1%) of the general dentists did not have any formal training in pediatric dentistry practices. However, most (73.5%) of them showed a willingness to attend such workshops or training courses if and when offered.
Table 1. Frequency distribution of gender, years of experience, owning a dental practice, and availability of visiting pediatric dentist.
| Variables | Number | % | |
|---|---|---|---|
| Gender | Male | 88 | 47.6 |
| Female | 97 | 52.4 | |
| Years of experience | Less than 5 years | 114 | 61.6 |
| 5-10 years | 53 | 28.6 | |
| More than 10 years | 18 | 9.7 | |
| Availability of a visiting pediatric dentist | Yes | 49 | 26.5 |
| No | 136 | 73.5 | |
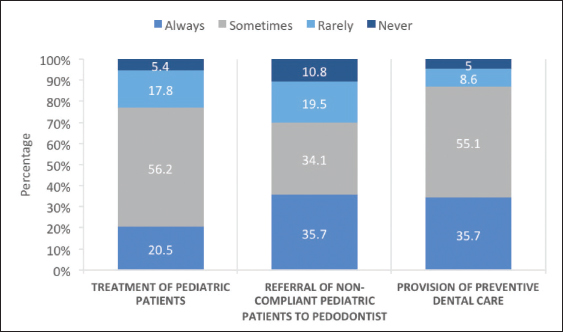
Figure 1. Frequency of treatment, referral, and provision of preventive dental care by the general dentists.
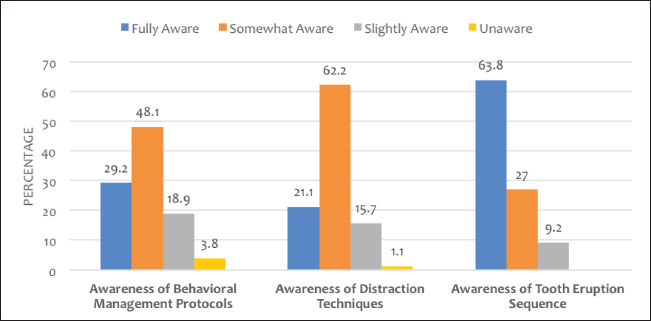
Figure 2. Awareness of behavioral management, distraction techniques, and tooth eruption sequence among the general dentists.
Discussion
Pediatric dental care is critical for ensuring oral health and, consequently, the general health of the children. General dentists are often the primary providers of dental services to children. Previous literature has suggested that most general dentists, ranging from 38% to 91%, were providing pediatric dental care in different parts of the world. However, referral to a pediatric dentist was made mostly in cases where the patient was younger than 4 years, had high caries experience, or was covered by a dental health insurance program.14-16 In the present study, most general dentists provided basic preventive and restorative dental services to pediatric patients and only referred uncooperative children to a pediatric dentist. The variations in practices related to dental treatment of pediatric population though exist among different countries/regions, there is, however, a propensity among general dentists to avoid the treatment of child patients.15,17 The ratio of general dentists to pediatric dentists is higher in developing than the underdeveloped countries.8,17 There is a limited number of specialized pediatric dentists available in Pakistan, compelling general dentists to play an extended role in providing dental care to children.13,17
Table 2. Use of different distraction techniques and their gender-wise comparison.
| Distraction techniques | Total use n (%) |
Male n (%) |
Female n (%) |
p-value |
|---|---|---|---|---|
| Visual (videos/kaleidoscope) | 57 (30.8) | 17 (19.3) | 40 (41.2) | 0.001 |
| Visual (Video games) | 57 (30.8) | 27 (30.6) | 30 (30.9) | 0.549 |
| Auditory (music) | 93 (50.3) | 39 (44.3) | 54 (55.6) | 0.081 |
| Virtual reality glasses | 26 (14.1) | 6 (6.8) | 20 (20.6) | 0.006 |
| Restraints | 94 (50.8) | 60 (68.1) | 34 (35) | 0.001 |
| Needle disguise | 65 (35.1) | 23 (26.1) | 42 (43.2) | 0.011 |
| Toys | 112 (60.5) | 64 (72.7) | 48 (49.4) | 0.001 |
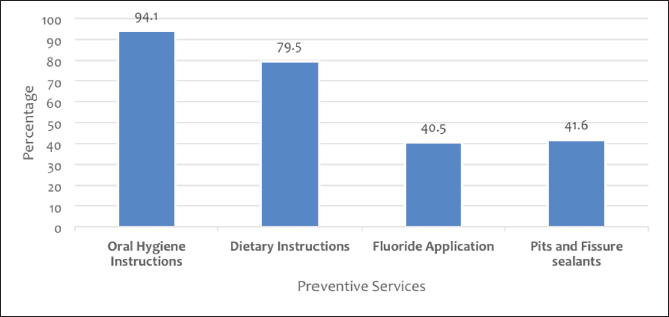
Figure 3. Various preventive services offered by general dentists to pediatric patients.
The quality of dental care provided to pediatric patients by general dentists varies significantly.8 One study conducted in New York found that general dentists often offer pediatric dental care that does not meet the AAPD standard of practice.18 Another study found that only 14% of general dentists follow the AAPD guidelines for fluoride varnish application and only 12% for fissure sealants.16,19 On the other hand, studies have shown that general dentists can provide pediatric patients with high-quality dental treatment.7,20 A US study revealed that dentists who had completed a residency were more likely to adhere to the AAPD guidelines for the administration of fluoride varnish and fissure sealants.21 In this study, most of the general dentists had not attended any formal training or courses in pediatric dentistry, yet they were treating pediatric patients for routine procedures. Furthermore, only one-third of dental clinics had visiting pediatric dentists available. However, most general dentists in the present study were willing to attend workshops or short courses to improve their clinical pediatric dentistry skills and provide services more effectively.
The dearth of preventive care offered to pediatric patients is a major cause for concern. According to the published studies, many general dentists do not provide children with preventive care like fluoride treatments, fissure sealants, and oral health education, which is a significant problem because preventive care is essential for preventing pediatric dental diseases.22,23 Among the preventive services, most of the dentists in the present study only provided oral hygiene instructions and dietary counseling. These results were not consistent with the previous studies carried out in the US and Europe.23-25 It is important to note that preventive services like topical fluoride applications, pit and fissure sealants, and preventive resin restorations can be provided by general dentists or dental hygienists.8,26 It is heartening to note that pediatric dentistry has recently been included as the fifth major subject in the final year of undergraduate dental training by the Pakistan Medical and Dental Council through their 2022 Standards currently in place for Academic Dental Institutions.27 However, unfortunately, the administration of most of the dental colleges is delaying the implementation of the decision, citing the cost involved in creating Pediatric Dentistry Departments and hiring Pediatric Dentistry Faculty.
Table 3. Frequency and comparison of treatment services provided in clinics with and without pediatric dentists.
| Treatment services | n (%) | Visiting pediatric dentist | p-value | |
|---|---|---|---|---|
| Yes n (%) | No n (%) |
|||
| Specialized pediatric dental units | 37 (20) | 18 (36.7) | 19 (13.9) | 0.001 |
| Specialized pediatric operating room | 34 (18.4) | 15 (30.6) | 19 (13.9) | 0.011 |
| Child-friendly attire | 59 (31.9) | 21 (42.8) | 38 (27.9) | 0.042 |
| Conscious sedation equipment | 17 (9.2) | 4 (8.1) | 13 (9.5) | 0.515 |
| Preventive services | 85 (45.9) | 24 (48.9) | 61 (44.8) | 0.370 |
| Management of trauma cases | 52 (28.1) | 12 (24.4) | 40 (29.4) | 0.322 |
| Space maintainers | 67 (36.2) | 26 (53) | 41 (30.1) | 0.044 |
| Scaling | 120 (64.9) | 34 (69.3) | 86 (63.2) | 0.645 |
| Fillings | 168 (90.8) | 47 (95.9) | 121 (88.9) | 0.121 |
| Pulpotomy | 122 (65.9) | 38 (77.5) | 84 (61.7) | 0.032 |
| Pulpectomy | 128 (69.2) | 38 (77.5) | 90 (66.1) | 0.096 |
| Extractions | 147 (79.5) | 42 (85.7) | 105 (77.2) | 0.144 |
| Stainless steel crowns | 53 (28.6) | 21 (42.8) | 32 (23.5) | 0.010 |
| Strip crowns | 14 (7.6) | 6 (12.2) | 8 (5.8) | 0.131 |
The findings of the present study demonstrated that general dentists are fully aware of the eruption sequence of primary teeth. However, they are not conversant with the methods of behavior guidance. Effective behavior management in pediatric dentistry requires understanding child psychology, developing rapport with young patients, and employing various techniques to manage anxiety and uncooperative behavior. Moreover, these skills are complex and require dedicated training and practice, which general dentists may not have extensively covered in their initial dental education.28 It is imperative that general dentists are trained in behavior guidance techniques to successfully serve their pediatric patients. Distraction is a simple and effective technique that can be used with any child, regardless of their level of cooperation.29 Most respondents in the present study claimed to use distraction strategies, with auditory distraction and toys being the most frequently used modalities, whereas the latest distraction techniques, such as VR glasses, were reported to be used least frequently.
The pediatric population roughly constitutes around 43% of the total population in Pakistan.30 Keeping in view the scarce availability of Pediatric Dentists in the country, the general dentists have to provide preventive and restorative services to our pediatric population. The Pakistan Academy of Pediatric Dentistry has expressed serious concerns about the situation.17
Future research should aim to include a larger and more diverse sample of dentists, encompassing both general and specialized practitioners from various regions to enhance the generalizability of the findings. Establishing mandatory continuing education programs and workshops for general dentists will ensure they are equipped with the latest knowledge and skills to manage pediatric dental care effectively.
Conclusion
A notable knowledge gap regarding the use of behavior management techniques exists in the general dentists that are mostly treating the pediatric dental patients in private dental care settings. However, there is a strong willingness among general dentists to engage in further trainings and workshops in pediatric dentistry to cater this large set of vulnerable populations in their daily practice.
Limitations of the study
The study’s limitations include its cross-sectional design and limited sample size, which provides a snapshot rather than longitudinal insights. The sample size, focused solely on general dentists in Lahore, which limits generalizability. The study was limited to Lahore, which may have different healthcare infrastructure and practices compared to other cities and rural areas in Pakistan. Future research should encompass a more diverse and extensive sample and a longitudinal design.
Acknowledgement
The authors would like to acknowledge all the dentists who participated in this questionnaire-based survey and provided us with the relevant information.
List of Abbreviation
| AAPD | American Academy of Pediatric Dentistry |
Conflict of interest
None to declare.
Grant support and financial disclosure
None to disclose.
Ethical approval
The ethical approval was obtained from the Institutional Review Board of Institute of Dentistry, CMH Lahore Medical College on 13-12-2022 vide Letter No 720/ERC/CMH/LMC.
Authors’ contribution
MJ: Conceptualization and design, acquisition and interpretation of data, drafting of manuscript.
AHW: Critical intellectual input, interpretation of data
HH: Acquisition and analysis of data, drafting of manuscript, critical intellectual input.
ALL AUTHORS: Approval of the final version of the manuscript to be published.
Authors’ details
Memoona Javed1, Amjad H Wyne2, Hammad Hassan3
- Demonstrator, Pediatric Dentistry Department, Institute of Dentistry, CMH Lahore Medical College, National University of Medical Sciences, Islamabad, Pakistan
- President, Consultant Pediatric Dentist, Pakistan Academy of Pediatric Dentistry, Lahore, Pakistan
- Assistant Professor, Science of Dental Materials Department, University of Health Sciences, Lahore, Pakistan
References
- Hassan H. Incidence of oral hygiene status and practices among children. Pak J Sci. 2021;73(1):35–9. https://doi.org/10.57041/pjs.v73i1.648
- Khan FR, Mahmud S, Rahman M. The need of paediatric dentistry specialists in Pakistan. J Coll Physici Surg Pak. 2013;23(4):305.
- Hamid S. Oral Health Disparities in 6-9 years old Pakistani School Going Children. Oral Health. 2019;7(01):1–6.
- Hassan H, Zaidi ZF, Shakoor A, Asad R, Fatima R, Mir B. Oral hygiene practices of rural and urban school going children in Punjab. Natl J Health Sci. 2024;9(1):29–32. https://doi.org/10.21089/njhs.91.0029
- Baliga S. Emerging trends in pediatric dentistry. J Indian Soc Pedod Prev Dent. 2018;36(2):107. 10.4103/JISPPD.JISPPD_171_18
- Taqi M, Zaidi JA, Shaikh H, Sukkurwalla A. Establishing dental recall interval for Pakistani children: a longitudinal study. J Pak Med Assoc. 2021;71(7):1799–803. https://doi.org/10.47391/JPMA.137
- Surdu S, Dall TM, Langelier M, Forte GJ, Chakrabarti R, Reynolds RL. The pediatric dental workforce in 2016 and beyond. J Am Dent Assoc. 2019;150(7):609–17. e5. https://doi.org/10.1016/j.adaj.2019.02.025
- McKnight-Hanes C, Myers D, Davis H. Dentists’ perceptions of the variety of dental services provided for children. ASDC J Dent Child. 1994;61(4):282–4.
- Perazzo MF, Otoni ALC, Costa MS, Granville‐Granville AF, Paiva SM, Martins‐Júnior PA. The top 100 most‐cited papers in paediatric dentistry journals: a bibliometric analysis. Int J Paediatr Dent. 2019;29(6):692–711. https://doi.org/10.1111/ipd.12563
- Coté CJ, Wilson S, Pediatrics AAo, Dentistry AAoP. Guidelines for monitoring and management of pediatric patients before, during, and after sedation for diagnostic and therapeutic procedures. Pediatrics. 2019;143(6):1–31. https://doi.org/10.1542/peds.2019-1000
- Ezzeldin M, Hanks G, Collard M. United Kingdom pediatric dentistry specialist views on the administration of articaine in children. J Dent Anesth Pain Med. 2020;20(5):303–12. https://10.17245/jdapm.2020.20.5.303
- Khan FR, Mahmud S, Rahman M. Pediatric dentistry training for dentists in Pakistan. J Pak Dent Assoc. 2013;22(1):03–8.
- Zalan AK, Qazi S, Zahid N, Haq A, Memon Z, Anser M. Attitude and practice of general dental practitioners and other dental specialties towards pediatric dentistry in Pakistan. J Pak Dent Assoc. 2022;31(1):17–21. https://10.25301/JPDA.311.11
- Sales SC, Meyfarth S, Scarparo A. The clinical practice of pediatric dentistry post-COVID-19: the current evidences. Pediatr Dent J. 2021;31(1):25–32. https://doi.org/10.1016/j.pdj.2021.01.002
- Wali A, Siddiqui TM, Khan R, Batool K. Knowledge, attitude, and practices of dental surgeons in managing child patients. Int J Clin Pediatr Dent. 2016;9(4):372–78. https://10.5005/jp-journals-10005-1393
- Aburahima N, Hussein I, Kowash M, Alsalami A, Al Halabi M. Assessment of paediatricians’ oral health knowledge, behaviour, and attitude in the United Arab Emirates. Int J Dent. 2020;2020(1):7930564. https://doi.org/10.1155/2020/7930564
- Jawaid SA. Plight of dentistry in Pakistan. Pak J Med Sci. 2020;36(3):299–302. https://10.12669/pjms.36.3.2278
- Maloney WJ. America, We need to invest in dental care for all of our children. New York State Dent J. 2022;88(1):14–7.
- Jordan KS, Steelman SH. Implementing safe and effective pediatric procedural sedation in the emergency department. Adv Emerg Nurs J. 2021;43(4):293–302. https://10.1097/TME.0000000000000380
- Adyanthaya A, Sreelakshmi N, Ismail S, Raheema M. Barriers to dental care for children with special needs: general dentists’ perception in Kerala, India. J Indian soc Pedod Prev Dent. 2017;35(3):216–22. https://10.4103/JISPPD.JISPPD_152_16
- Wright JT, Crall JJ, Fontana M, Gillette EJ, Nový BB, Dhar V, et al. Evidence-based clinical practice guideline for the use of pit-and-fissure sealants: a report of the American Dental Association and the American Academy of Pediatric Dentistry. J Am Dent Assoc. 2016;147(8):672–82. e12. https://doi.org/10.1016/j.adaj.2016.06.001
- Ogretme MS, AbualSaoud D, Hosey M. What preventive care do sedated children with caries referred to specialist services need? Br Dent J. 2016;221(12):777–84. https://doi.org/10.1038/sj.bdj.2016.951
- Aljafari A, ElKarmi R, Kussad J, Hosey M. General dental practitioners’ approach to caries prevention in high-caries-risk children. Eur Arch Paediatr Dent. 2021;22:187–93. https://doi.org/10.1007/s40368-020-00548-4
- Bonetti D, Clarkson JE. Fluoride varnish for caries prevention: efficacy and implementation. Caries Res. 2016;50(Suppl. 1):45–9. https://doi.org/10.1159/000444268
- Hadjipanayis A, Grossman Z, Del Torso S, Michailidou K, Van Esso D, Cauwels R. Oral health training, knowledge, attitudes and practices of primary care paediatricians: a European survey. Eur J Pediatr. 2018;177:675–81. https://doi.org/10.1007/s00431-018-3108-z
- Davidson KW, Barry MJ, Mangione CM, Cabana M, Caughey AB, Davis EM, et al. Screening and interventions to prevent dental caries in children younger than 5 years: US preventive services task force recommendation statement. JAMA. 2021;326(21):2172–8. https://10.1001/jama.2021.20007
- istan Medical and Dental Council (PMDC).Guidelines for undergraduate dental education curriculum (BDS) 2022. Available from: https://pmc.gov.pk/Documents/Examinations/Guidelines%20for%20undergraduate%20Dental%20Education%20Curriculum%20(BDS).pdf
- Wright GZ, Kupietzky A. Behavior management in dentistry for children. Hoboken, NJ: John Wiley & Sons; 2014.
- Hassan H, Hassan SA, Razzaq A, Edrees M, Yaasir Z, Shakoor A. Impact of virtual reality goggles as a distraction technique on the pain perception and heart rate of pediatric dental patients. Journal of the Dow University of Health Sciences (JDUHS). 2023;17(3):136–41. https://doi.org/10.36570/jduhs.2023.3.1949
- Ahmed S, Haider S, Bokhari S. Prevalence of oral diseases in pediatric population in Karachi, Pakistan-a cross-sectional survey. J Dent Health Oral Disord Ther. 2017;6(1):00189. https://10.15406/jdhodt.2017.06.00189
Keywords: Dental care, general dentists, pediatric dentistry, dental treatment.

Publication History
Received: March 03, 2024
Revised: May 20, 2024
Accepted: June 14, 2024
Published: June 25, 2024
Authors
Memoona Javed
Demonstrator, Pediatric Dentistry Department, Institute of Dentistry, CMH Lahore Medical College, NUMS
Amjad H Wyne
President, Pakistan Academy of Pediatric Dentistry
Hammad Hassan
Assistant Professor, Dental Materials Department, University of Health Sciences, Lahore